Do you know about New Zealand’s International Travel Vaccination Certificate? Me neither!
It’s a little mysterious. I’m not sure if the government knows that much either. If officials do know about this so-called certificate, they’re not too keen to (transparently) share what they might know.
I’m aware there is a certain kind of moral and legal jeopardy – imbued perhaps with a touch of tyranny, if the New Zealand government were to lock in a requirement for an International Travel Vaccination Certificate (ITVC). You see, the state has known for quite some time that the vaccine couldn’t prevent transmission of infection.
Waves of reinfections are pounding the very New Zealanders who complied and were vaccinated, rather than lose their jobs. Rather than discuss early treatments which prevent the intensity and duration of infection, the government is now talking about a plan to restore quarantine.
In this concerning, yet contradictory environment, my interest was piqued when I noticed on the New Zealand government Proof of COVID-19 vaccination status page, that
‘If you are travelling overseas and must show proof of your COVID-19 vaccination status, you need an International Travel Vaccination Certificate.’
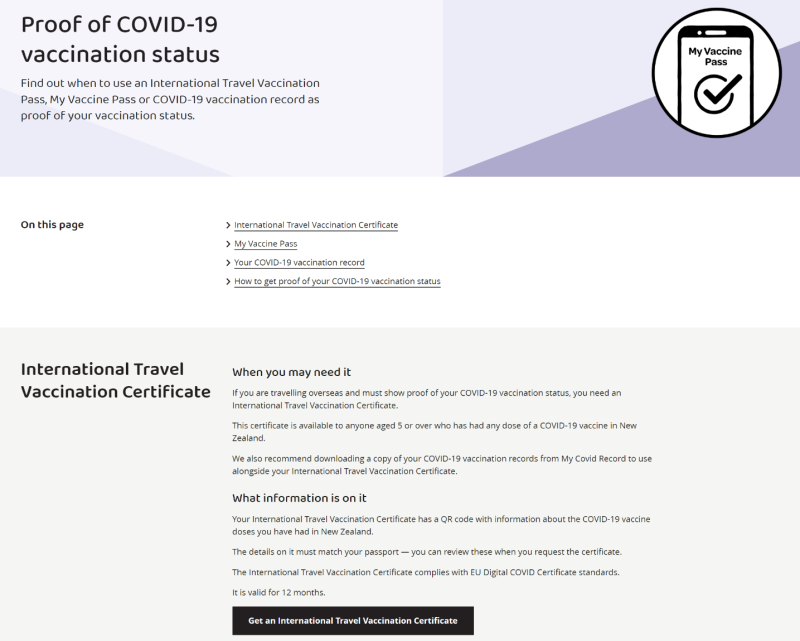
I wondered what this was, what it might entail, and what other countries might have a certificate locked so effectively into policy.
I couldn’t see any broad policy-based discussion, so on September 22, 2022, I made Official Information Act requests to the Department of the Prime Minister and Cabinet (Jacinda Ardern’s department, the DPMC) and the Ministry of Health.
I wanted to understand what information was held internally by agencies and government officials, including information and advice received from the WHO, United Nations agencies, from GAVI and CEPI; from the World Economic Forum as well as from management consultancy firms.
Because, after all, the ITVC infers that it is COVID-19 that is the risk. Therefore, to comply, the public receives a novel mRNA gene therapy that instructs the body to replicate an antigenic, inflammatory spike protein. The Ministry of Health has recently removed an OIA request document that described New Zealand clinical evaluation information – including the description of the ‘nucleoside-modified messenger RNA encoding the SARS-CoV-2 S-glycoprotein.’
I.e. – The compliance demands receipt of a biotechnology that codes instructions for the body to reproduce the Spike (S) protein. Does New Zealand civil society know that the COVID-19 ‘vaccine’ was in fact single-stranded messenger RNA (mRNA) which coded for full-length, codon-optimised, pre-fusion stabilised conformation variant (K986P and V987P) of the SARS-CoV-2 spike (S) glycoproteins (the antigen)?
With no off-switch?
In response the DPMC provided me with a single document: the 23 March 2021 NAB Assessment Report (AR 086/2020-21): COVID-19 Vaccines: Managing the Borders. This was produced in the same month the all-citizens-injected rollout strategy was declared.
Page four is enlightening.
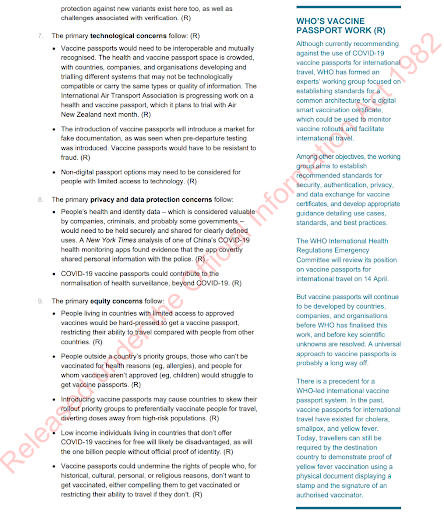
The section, ‘WHO’s Vaccine Passport Work’ demonstrates how effortless the presumption was, in March 2021 – that vaccine passports would become a reality – i.e. set in law. The document is produced by the National Assessments Bureau, which is part of the New Zealand Intelligence Community.
The presumption is that you can’t fly unless you’ve received the single-stranded messenger RNA (mRNA) which coded for full-length, codon-optimised, pre-fusion stabilised conformation variant.
In addition, ‘Primary Equity Concerns’ appear blithe and legally uninformed.
The ‘equity concerns’ briefly touch on the potential for vaccine passports to undermine the rights of people who ‘for historical, cultural, personal, or religious reasons, don’t want to get vaccinated.’
They forgot (or neglected) to mention that people might not want to get vaccinated for scientific reasons. Among them might be the history of public trust, and informed consent, and the fact that this was a novel drug which is yet to complete clinical trials.
Can scientific reasons be downplayed, and largely dismissed as a personal reason? They might not want to get vaccinated because the respiratory virus never posed a risk to them, or their families, from day one. They might not want to get vaccinated because of a changing risk-benefit profile, because the safety signals exceed any benefits.
But such considerations weren’t within the scope of this rhetoric.
Official Information Act requests pushed out
My OIA request question to the DPMC:
Please advise all known countries who have integrated International Travel Vaccination Certificate into their policies and procedures currently, and countries for which this plan is underway.
Was denied:
I am refusing this part of your request under section 18(g)(i) of the Act, as the information requested is not held by DPMC, and I am advised it is not held by another department.
It was denied because one of the two key agencies enrolled in the rollout has no idea of any other country employing an ITVC.
The response infers that there is no ongoing discussion nor review of the global position on ITVC’s – yet on the Ministry of Health’s COVID-19 campaign website, such a travel instrument is presented as ordinary, or normal.
Following the request to the Ministry of Health, they partially transferred the request to the Ministry of Foreign Affairs (MFAT) on October 6. A fortnight later the Ministry of Health elected to extend the period of time available to the 22nd of November, as ‘further consultation is required.’
The MFAT considered that my request
as currently framed would capture a significant volume of information. As such, it was likely that my request will be refused under section 18(f) of the OIA, as it would have required substantial collation and research.
Crickey! This was surprising, as there are no public facing policy documents discussing this, and apart from references to the certificate, there is no more information online. As such, I agreed to refine my request from MFAT to Cabinet Papers, Memoranda and Reports prepared by MFAT and sent to the Minister of Foreign Affairs.
I insisted on retaining the original question requesting a list of the countries who have integrated International Travel Vaccination Certificate into their policies and procedures currently, and countries for which this plan is underway.
However this was also apparently too onerous and was extended to the 9th of December, 2021.
because consultations necessary to make a decision on your request are such that a proper response cannot reasonably be made within the original time frame (section 15A(1)(b) of the OIA refers).
As the OIA request response showed in March 2021, the authorities were assuming vaccine passports and certificates would become de rigueur, and ‘change the face of COVID-19 border management.’
Such a claim appears a wee bit predetermined.
The enthusiasm for an International Travel Vaccination Certificate is not backed up by independent science, which could review the safety and efficacy of a vaccine to ensure that manufacturers’ claims were triangulated – in the public interest. Throughout their COVID-19 campaign, the New Zealand government never made a place for science which might contradict prevailing policy.
COVID-19 information flowed in a weblike, networked manner across local agencies, the World Health Organisation, chief science advisors, vaccine lobbyists and regulatory agencies.
But science resourcing to verify corporate claims was never at arm’s length from the agencies with the vested political interest.
New Zealand’s all-citizens-injected policy
The push for universal vaccination was decided at a very high level. It is evident that Queen Elizabeth II desired that the entire New Zealand population was vaccinated. The Pfizer contract for enough doses for the entire population was signed by the Sovereign in right of New Zealand, our then head of state (Queen Elizabeth II). The all-citizens-injected rollout strategy was established in March 2021. It’s clear that Prime Minister Ardern and the Hon Chris Hipkins were intimately involved in the deployment, reporting both the signing of the contract and the arrival of the first batches.
So-called evidence of vaccine safety and efficacy revolved around the administration and analysis of the evidence supplied by Pfizer, based on the manufacturer complying with the 58 conditions of the provisional consent notice. Pfizer was required to provide ‘monthly safety reports, as well as all safety reviews they conduct or become aware of.’ In addition, condition 54 required the manufacturer to:
Provide any reports on efficacy including asymptomatic infection in the vaccinated group, vaccine failure, immunogenicity, efficacy in population subgroups and results from post-marketing studies, within five working days of these being produced.
Gaps appear. It seems that Pfizer might not have supplied their February 2021 post-marketing report to the Ministry of Health in a timely manner. When asked in October 2021 for post-marketing reports, the Ministry responded ‘reports you seek regarding condition 54 do not exist.’
(An alternative explanation is that they are technically refusing to acknowledge the Feb report as relevant to [54] as [54] did not specifically state safety reports.)
Contradictions and inconsistencies could never stop the rollout
Knowledge gaps, conflicts of interests and contradictions permeated New Zealand government memos and modeling papers. State-approved information providers were always under the auspices of the agencies which were responsible for implementing and delivering the vaccine strategy.
Task forces were designed to support the rollout, not undermine it. The primary New Zealand Ministry of Health scientific vehicle – the Vaccine Strategy Science and Technical Advisory Group (CV-TAG) – was designed to provide advice to the COVID-19 Vaccine Strategy Taskforce on the use of COVID-19 vaccinations. The chair was Chief Science Advisor to the Ministry of Health, Ian Town. The COVID-19 Vaccine Strategy Taskforce was established to oversee implementation of the vaccine strategy. The CV-TAG was hardly likely to contradict their own agency’s locked in programme.
The memos produced by the CV-TAG demonstrate that methodological analyses of the scientific literature were not undertaken, either to triangulate Pfizer’s data or to look at non-vaccine alternatives.
Jacinda Ardern’s DPMC-funded modeling group Te Pūnaha Matatini/Covid-19 Modelling Aotearoa received NZD2 million between September 20, 2021 and June 30, 2022. It was unlikely they would compromise the campaign.
The most senior modelers (a professor of mathematics and statistics, an expert in physics and complexity, and a graduate of finance-based computational and applied mathematical sciences) claimed that vaccination is the only way to achieve population immunity.
Before mandates rained down on civil society, scientists knew the injection was not effective.
By June 2021 a senior group contradicted itself by advising the Minister of Health that vaccine-achieved herd immunity was unlikely and that variants would continue to escape – yet that the elimination strategy would be feasible through a successful vaccine campaign. The paper was embargoed from public view for two months, and the public were never advised that “likely levels of vaccination coverage… will not be sufficient to cross the herd immunity threshold.”
Covid-19 Modeling Aotearoa modelers in August 2021 were aware that the injection would not prevent ongoing infection – they modeled a baseline vaccine efficacy as a 70% reduction in infection, 50% reduction in onward transmission for those who get infected.
Yet still, in line with the March 2021 strategy, the Minister for COVID-19, Chris Hipkins systematically rolled the mandates out. In October affected workers over 12 had to be injected, and by December 3 you couldn’t go to the gym, the swimming pool or a national park unless you had agreed to code the spike protein inside your body.
Reinfections after widespread compliance
The Ministry of Health’s Chief Science Advisor and chair of the CV-TAG knew in September that boosters on immunocompromised groups were unreliable.
As of this writing, reinfection waves keep pounding Kiwis. They’re mystified. They were never adequately informed that vaccine-associated enhanced disease (VAED), including vaccine associated enhanced respiratory disease (VAERD) was logged by the manufacturer as an ‘important potential risk.’
The European regulator stated:
there is a theoretical risk, mostly based on non-clinical betacoronavirus data, of VAED occurring either before the full vaccine regimen is administered or in vaccinees who have waning immunity over time. If VAED were to be identified as a true risk, depending on its incidence and severity, it may negatively impact the overall vaccine benefit risk assessment for certain individuals.
But New Zealand is captured. There is no scientific community with sufficient latitude and resourcing to conduct any research that explores this relationship, or conduct any research which might challenge safety and efficacy claims made by Ministers of the Crown, elected officials and media.
How can the governed trust the governors?
Of course, to maintain trust, officials and elected members in democracies must be democratically accountable to civil society. Their claims should be evidence-based and backed up by unbiased information (including independent science), that is free from conflicts of interest. These actors have an overriding obligation to protect health and keep people safe. This is how trust in the governors is sustained over time.
The utilitarian ‘greater good’ mandates were entirely contradicted by these (quietly held) institutional knowledges – before the mandates were produced.
The Hon Minister Hipkins currently refuses to answer OIA requests relating to his time in this position, despite being responsible for the mandate’s legislation.
Many of us are familiar with the magic of substantial equivalency, the magic that enables chemicals, potions and new biotechnologies to slip through the fingers of regulatory agencies, to then be released onto the market for public consumption.
We now see Big Pharma is using antibody titres (levels) from clinical trials to prove a vaccine ‘works.’
Immunobridging is the next substantial equivalency trick – where neutralising antibody concentrations and seroresponse rates signal that maybe the immune system can put up enough of a defence to prevent something. Why do I say ‘something?’ Well, efficacy in the original Pfizer mRNA BNT162b2 trials wasn’t signalled by prevention of hospitalisation and death; this was simply inferred by less symptoms at 7 days post dose 2. The infamous 95% efficacy claim, repeated ad nauseum, was based on this tremendously short time interval.
Now they have the gall to infer that immunobridging response in one age group will be reflective of the response in a slightly different age group.
The ludicrous stupidity of vaccine passports for a rapidly mutating respiratory virus is patently clear for anyone with either awareness of the history of public health and epidemiology, or who is a primary care physician and understands the limits of vaccines – particularly for patients with complex chronic health conditions. Everyone is different. Everyone responds differently to both viruses and medication.
Our government knew efficacy in the clinical trials vastly misrepresented the claims they made to the public. They knew the vaccine didn’t prevent transmission, that it couldn’t be confirmed to protect the most vulnerable. Yet still they rolled on with authoritarian, lockstep universal mandates. Now we have new substantial equivalency tricks.
Yet still New Zealand government public-facing websites infer that International Travel Vaccination Certificates are a reasonable, legitimate, and ethical instrument of regulation and control.
They’re not.
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.