In the interests of transparency and to help readers form their own judgments of potential bias, Nature Portfolio journals require authors to declare any competing financial and/or non-financial interests in relation to the work described. ~ nature portfolio > editorial policies > competing interests
This is a story of an author who promoted COVID-19 vaccine uptake among adolescents while failing to disclose significant competing interests (e.g., his holding of an unrestricted research grant from Pfizer). This is also a story of a failure of the author’s publisher Nature Reviews Cardiology to enforce Nature Portfolio’s declaration-of-competing-interests policy. Finally, this is a story of a failure of Nature Reviews Cardiology’s editorial- and peer-review process to correct an author’s bias reflecting the author’s competing interests.
As I was reading an article titled “Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms” in Nature Reviews Cardiology, I noted the lack of supporting references for some the author’s claims, such as “[W]ith COVID-19 vaccination, the risk of myocardial injury and myocarditis decreases 1,000-fold in the general population ….” For other claims, the references supplied did not support the claims made. In addition, the tone of the article was one of ardent promotion of COVID-19 vaccination; e.g., a section title reads “Vaccinations: the way to go!” I decided to investigate whether the author had undisclosed competing interests. That investigation led to my submitting 28 March 2023 a “Correspondence article” to the editors of Nature Reviews Cardiology.
My Submission to Nature Reviews Cardiology (slightly edited):
I write to inform the readers and editors of Nature Reviews Cardiology of significant, undisclosed competing interests of the lead author, Stephane Heymans, of “Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms” [1] (Nat. Rev. Cardiol. 19, 75–77 (2022)), a Comment article published online 9 December 2021. The “Ethics Declaration” of Heymans’ Comment article reads, “The authors declare no competing interests.” However, Heymans’ conflict-of-interest statement for an article [2] first published 30 December 2021 (submitted 1 September 2021) reads, “S.H. received personal fees for scientific advice from AstraZeneca, CSL Behring, Cellprothera, Bayer and Merck; and an unrestricted research grant from Pfizer.” Heymans’ LinkedIn profile [3] concludes, “[H]e advices [sic] different biotech and pharmaceutical companies, as well as venture capital firms looking for the best investments.”
Heymans’ conflicts of interest are clearly relevant to his Comment-article exhortations such as “Vaccinations: the way to go!” Furthermore, Heymans’ Comment article provides evidence of author bias:
- The assertion “Among patients with COVID-19, 10% of outpatients and 40% of hospitalized patients have clinically significant myocardial injury, mostly in the absence of clinically significant coronary artery disease” is not supported by the cited reference [4], which does not discuss the absence of coronary-artery disease; rather, it states, “Although the mechanism of myocardial injury associated with COVID‐19 is not completely understood, patients with cardiovascular disease are four times [as] likely to have elevated hs‐cTn levels than those without [hs-cTn = high‐sensitivity cardiac troponin, elevated levels suggesting injury].”
- The assertion “To date, only eight deaths owing to COVID-19 mRNA-vaccine-associated myocarditis have been reported … (see Supplementary information)” is not supported by the supplementary information, a list of 159 references, the majority relating to vaccine-associated myocarditis “VAM.” Reference 79 reports 8 Pfizer mRNA VAM deaths (European Medicines Agency data), as well as 2 Pfizer VAM deaths announced by Israel’s Ministry of Health April 2021. References 1, 25, and 147 report, respectively, the following mRNA VAM deaths: 27-year-old male (Pfizer, USA), 22-year-old male (Pfizer, Korea), 42-year-old male (Moderna, USA). Thus, the total number of reference-list-reported mRNA-VAM deaths is at least 13, not the claimed 8.
- The supplementary reference list is also used to support the claim: “In COVID-19 mRNA-vaccine-associated myocarditis, >90% of patients will functionally completely recover ….” However, it’s not clear which reference or group of references provide support. In fact, reference 79 contradicts the claim, reporting “Although rare, the identified association can be serious as shown by the finding that a large proportion of cases did not recover and by the (albeit few) fatalities.” A Nature-Medicine article [5], published online 14 December 2021, reports 158 Pfizer VAM cases (Table 2), with 25 leading to death (Table S1), yielding a survival rate of approximately 84.2% (not >90% complete recovery).
- Finally, no supporting references are provided for some assertions, such as “[W]ith COVID-19 vaccination, the risk of myocardial injury and myocarditis decreases 1,000-fold in the general population ….”
End of Submission
On 14 April 2023, Nature Reviews Cardiology’s chief editor Dr. Gregory Lim forwarded to me a polite response from Dr. Heymans to my submitted Correspondence article in which Heymans acknowledged his “current advisory roles with AstraZeneca and CSL Behring” while failing to acknowledge his unrestricted research grant from Pfizer as well as failing to address potential competing interests relating to his work as an investment advisor. Dr. Heymans also responded to my bullet points (see below). Editor Lim stated, “As we feel that Professor Heymans has satisfactorily addressed your comments, and no corrections to the Comment article are required, we have decided not to proceed with publication of your Correspondence.”
Shouldn’t a competing-interests disclosure-policy compel an author promoting a product produced by Pfizer and AstraZeneca to disclose he has an unrestricted research grant from Pfizer and serves as an advisor to AstraZeneca? I claim that Nature Portfolio’s policy does require such a disclosure. Before I validate this claim, see if you agree with Editor Lim that Professor Heymans has satisfactorily addressed my bullet-point comments.
Bullet Point 1: Dr. Heymans responded to my first bullet point by stating “Some references did not completely cover the statements [owing to a reference limit of 10 for Comment articles].” However, the reference he supplied [4] does not even partially cover his claim that patients with COVID-19 have clinically significant myocardial injury “mostly in the absence of clinically significant coronary artery disease.” This claim is misleading for two reasons—(i) the reference cited does not make this claim at all; rather, (ii) it suggests the opposite is true with “coronary artery disease” replaced by the broader “cardiovascular disease.”
Bullet Point #2: Dr. Heymans’ response concludes
We based this number [8 VAM deaths reported to date] mainly on the following publication, but indeed knowledge may have changed since then, and after our publication.
Lazaros G, Klein AL, Hatziantoniou S, Tsioufis C, Tsakris A, Anastassopoulou C. The Novel Platform of mRNA COVID-19 Vaccines and Myocarditis: Clues into the Potential Association. [published online ahead of print, 2021 Jul 13]. Vaccine. 2021. doi.org/10.1016/j.vaccine.2021.07.016
In my bullet point I did not refer to “knowledge” that changed “after publication.” Rather, I referred to information in Dr. Heymans’ own list of references! The specific reference Dr. Heymans cites (Lazaros et al.) discusses 10 VAM deaths (8 in Europe and 2 highly publicized deaths in Israel) and, as I have detailed, Dr. Heymans’ reference list includes a discussion of at least 3 more VAM deaths. Why would Dr. Heymans wish to underreport VAM-death incidence? Might it be related to his competing interests as a pharmaceutical industry advisor and as a recipient of an unrestricted research grant from Pfizer?
Bullet Point #3: Here is Dr. Heymans’ response:
We based our estimation [> 90% on different publications. The functional recovery refers to the cardiac function, the improvement of systolic function (ejection fraction), not to the number of events. The interesting publication Dr. Bourdon is referring to, is confusing, as it also looks at post-vaccine events in those patients that had been hospitalized only (selection bias), also including patient (sic) having both the vaccine and the COVID-19 infection.
Even in Dr. Heymans’ response, we do not find any specific references that support his estimate of > 90% functional recovery from VAM. Note that I have provided two references that don’t support his estimate—one is a reference (Lazaros et al.) that Dr. Heymans provided in [1], which finds a “not recovered/not resolved” rate of 30.6% for Moderna’s mRNA-1273 and 33.2% for Pfizer’s BNT162b2. I do realize that my second reference ([5])was not published until shortly after [1] appeared.
Regarding Dr. Heymans’ comments about Patone et al.’s publication [5]: yes, the 158 Pfizer VAM events observed in Patone et al.’s study population were indeed all hospitalized owing to VAM. A recent meta-analysis of 23 vaccine-associated myocarditis/pericarditis studies including 854 patients ages 12-20 years found a 92.6 percent case-hospitalization rate with a mean length of stay of 2.8 days and a 23.2 percent ICU admission rate. So, to adjust for selection bias, we might estimate that Patone et al.’s 158 Pfizer VAM events requiring hospitalization were drawn from 158/0.926≈171 VAM events. There were 25 deaths resulting from these events (with 13 of the events being hypothetical). This leads to a survival rate of about 85.4 percent (≈171-25/171)*100%); again, not > 90 percent functional recovery. Even a 70 percent VAM hospitalization rate would lead to a survival rate of under 90 percent (88.9 percent).
Bullet Point #4: The complete sentence from [1] that includes Dr. Heymans’ unsupported assertion highlighted in my fourth bullet reads, “Moreover, with COVID-19 vaccination, the risk of myocardial injury and myocarditis [associated with infection] decreases 1,000-fold in the general population, with a minor 1–5-fold increased risk of mild myocarditis in young adults [associated with vaccination]” (clarifying bracketed comments and boldface type added by me). Here is Dr. Heymans’ response:
This statement results from a calculation following literature. Taking myocardial injury and myocarditis together after COVID infection (because in clinical practice troponin elevation from myocardial injury due to severe illness or myocarditis have similar presentations), incidence is 1000-4000 per 100,000 after COVID-19 infection. Incidence of myocarditis/myocardial injury is 1-10 per 100,000 in vaccinated people. That’s why we came to this statement of 1000 fold. Vaccination is consistently associated with lower risk of major adverse cardiac events after COVID infection (1, 2).
In the first four sentences of his response, Dr. Heymans appears to be making the same apples-to-oranges comparison that he makes in Table 1 of his published article [1]:
Except from Table 1 of [1]
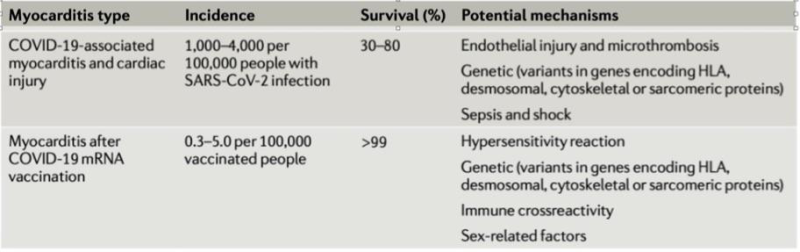
In the preceding table, Dr. Heymans is comparing infection-related risk of “myocarditis and cardiac injury” to myocarditis risk only related to vaccination. He should either be comparing infection-associated myocarditis incidence to vaccine-associated myocarditis incidence or infection-associated myocarditis-and-cardiac-injury incidence (signaled by elevated troponin levels) to vaccine-associated myocarditis-and-cardiac-injury incidence. Either of these valid (unbiased) comparisons would show rates are comparable (ratio roughly = 1, not 1,000).
For example, a study by Mansanguan et al. finds evidence of cardiac injury (elevated troponin levels) following Pfizer BNT162b2 at rate of 2,475 per 100,000 vaccinated adolescent males (in the range 1,000-4,000 that Dr. Heymans gives for post-infection cardiac injury). Another study by Dr. Christian Mueller (University Hospital Basel) finds 22 of 777 mRNA booster-dose recipients had resulting adjudicated myocardial injury (signaled by elevated troponin levels), corresponding to a rate of 2,831 per 100,000 (with a higher rate among females than among males). As for myocarditis risk post-infection, Karlstad et al. (eTable 7) find the risk of infection-related myocarditis to be, for males 12+, about 3.69 cases per 100,000 infections per 28 days (risk period post infection) and about 3.42 for females 12+. Compare these infection-associated rates to the VAM rate given in Dr. Heymans’ Table 1: 0.3 to 5 cases per 100,000 vaccinations.
Remark: VAM rates can be considerably higher than myocarditis rates associated with infection; e.g., Karlstad et al. find myocarditis incidence (requiring hospitalization) to be such that there are about 18 excess cases per 100,000 2nd doses of Moderna’s mRNA-1273 administered to males 16–24 while the rate associated with infection for 16–24 year-old males is 1.37 excess cases per 100,000 infections.
The only part of Dr. Heymans’ response that relates to his claim of vaccinations providing a “1,000-fold” decrease in myocardial-injury risk is its last sentence, in which Dr. Heymans provides two references to support the following much more modest assertion: “Vaccination is consistently associated with lower risk of major adverse cardiac events after COVID infection (1,2) [(1: Jiang et al, 2: Kim et al.)]”:
Jiang J, Chan L, Kauffman J, Narula J, Charney AW, Oh W, et al. Impact of Vaccination on Major Adverse Cardiovascular Events in Patients With COVID-19 Infection. J Am Coll Cardiol. 2023;81(9):928-30.
Kim YE, Huh K, Park YJ, Peck KR, Jung J. Association Between Vaccination and Acute Myocardial Infarction and Ischemic Stroke After COVID-19 Infection. JAMA. 2022;328(9):887-9.
First, I’ll point out that neither of the preceding references were available at the time of publication of Dr. Heyman’s Comment article [1]. Jiang et al. was published online 20 February 2023 and Kim et al. was published online 22 July 2022. More important is that Jiang et al.’s study of “Major Adverse Cardiac Events” (MACE) following COVID-19 infection does not support Dr. Heymans’ hyperbolic claim of a “1,000-fold” decrease in myocardial-injury risk derived from vaccination.
Jiang et al. find for their study population of 1,934,294 patients (with mean age 45.2 years) that full vaccination reduces the risk of infection-related MACE by an adjusted-hazard-ratio factor of 0.59 for the general population whereas Dr. Heymans has essentially suggested a factor of 0.001 for the general population. Park et al. find the hazard-reduction factor to be 0.42 (not 0.001).
Bottom line: Dr. Heymans has not provided any support whatsoever for his claim that “[W]ith COVID-19 vaccination, the risk of myocardial injury and myocarditis decreases 1,000-fold in the general population ….” In fact, he provides references suggesting his estimate of a “1,000-fold decrease” to be dramatically inflated.
I’ll now establish that Nature Portfolio’s declaration-of-competing-interests policy requires Dr. Heymans to disclose his competing interests.
Competing Interests: Nature Portfolio’s competing-interest policy conveys expectations of authors through definitions, including the following:
(1) “[C]ompeting interests are defined as financial and non-financial interests that could directly undermine, or be perceived to undermine the objectivity, integrity and value of a publication, through a potential influence on the judgements and actions of authors with regard to objective data presentation, analysis and interpretation.”
(2) “Financial competing interests include any of the following:”
(a) “Funding: Research support (including salaries, equipment, supplies, and other expenses) by organizations that may gain or lose financially through this publication.”
(b) “Employment: Recent (while engaged in the research project), present or anticipated employment by any organization that may gain or lose financially through this publication.”
(c) “Personal financial interests: Stocks or shares in companies that may gain or lose financially through publication; consultation fees or other forms of remuneration (including reimbursements for attending symposia) from organizations that may gain or lose financially; patents or patent applications (awarded or pending) filed by the authors or their institutions whose value may be affected by publication.”
∙ Dr. Heymans has a financial competing interest of type 2(a)—an unrestricted research grant from Pfizer whose mRNA vaccine he promoted in his Comment article [1]:
(i) The beginning paragraph of Dr. Heymans’ article [1] (set in boldface type) concludes “Therefore, COVID-19 vaccination should be recommended in adolescents and adults.”
(ii) A section header of [1] reads “Vaccinations: the way to go!” (also set in boldface type).
Now consider the extent to which Pfizer “may gain or lose financially through this publication,” where “this publication” is Dr. Heymans’ Comment article [1]. An analysis of Pfizer’s annual reports from 2021 and 2022 shows that for 2021, Pfizer’s mRNA COVID vaccine accounted for over 45% of the company’s revenue (36.781 billion of 81.3 billion). For 2022, Pfizer’s mRNA COVID vaccine accounted for over 37% of the company’s revenue (37.806 billion of 100.33 billion). How would Pfizer’s bottom line had been impacted had Dr. Heymans questioned the benefit-risk profile of mRNA COVID vaccination for young males (16-24, e.g.) who are at greatest risk of vaccine-associated myocarditis/pericarditis?
∙ Dr. Heymans has a financial competing interest of type 2(b)–his employment as an advisor to AstraZeneca.
Consider the following headline: “AstraZeneca to take profits from Covid vaccine” from a BBC article appearing about 1 month before the publication of Dr. Heymans’ article [1] in Nature Reviews Cardiology.
Furthermore, 2(b) mentions “anticipated employment by any organization that may gain or lose financially through this publication.” In general, a medical researcher endorsing the use of any pharmaceutical product is obligated to disclose any past, present, or anticipated future funding or income from the pharmaceutical industry. Why? A researcher interested in maintaining or attracting such funding may be unwilling to publish findings that do not support the consumption of pharmaceutical products.
∙ There is evidence that Dr. Heymans may have competing interests of type 2(c).
Dr. Heymans acknowledges in his LinkedIn profile that he advises “venture capital firms looking for the best investments.” Because Dr. Heymans offers investment advice, he must believe he has market insights that may benefit his clients. Given Dr. Heymans’ credentials and interests, it’s natural to assume his insights apply to investments in the pharmaceutical industry. An important question to consider: if Dr. Heymans’ clients have investments in the pharmaceutical industry, then would he be serving his clients’ interests were he to publish any statements potentially impacting the profitability of that industry?
Conclusion: In his Comment article [1], Dr. Heymans promoted uptake of COVID-19 vaccination with false, deceptive, unsupported, and exaggerated claims reflecting his competing interests (serving as an advisor to AstraZeneca, as well as other pharmaceutical companies, holding an unrestricted research grant from Pfizer, and providing advice on pharmaceutical-industry investments). Editor Lim failed to enforce Nature Portfolio’s competing-interest-disclosure policy. Moreover, for Dr. Heymans’ article [1] Nature Reviews Cardiology’s editorial- and peer-review process failed to correct author bias.
Note Bene: Dr. Joshua Parreco has pointed out Dr. Heymans’ coauthor Leslie T. Cooper also has undisclosed competing interests: according to OpenPaymentsData.cms.gov, Cooper received in December of 2021 consulting fees from both E.R. Squibb & Sons, L.L.C. and Moderna TX, Inc.
References
1. Heymans, S., Cooper, L.T. Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms. Nat Rev Cardiol 19, 75–77 (2022). https://doi.org/10.1038/s41569-021-00662-w
2. de Boer RA, Heymans S, Backs J, Carrier L, Coats AJS, Dimmeler S, Eschenhagen T, Filippatos G, Gepstein L, Hulot JS, Knöll R, Kupatt C, Linke WA, Seidman CE, Tocchetti CG, van der Velden J, Walsh R, Seferovic PM, Thum T. Targeted therapies in genetic dilated and hypertrophic cardiomyopathies: from molecular mechanisms to therapeutic targets. A position paper from the Heart Failure Association (HFA) and the Working Group on Myocardial Function of the European Society of Cardiology (ESC). Eur J Heart Fail. 2022 Mar;24(3):406-420. doi: https://doi.org/10.1002/ejhf.2414.
3. Stephane Heymans. LinkedIn Mini-Profile. https://be.linkedin.com/in/stephane-heymans-76528284?trk=author_mini-profile_title. Accessed 28 March 2023.
4. Aikawa, T., Takagi, H., Ishikawa, K. & Kuno, T. Myocardial injury characterized by elevated cardiac troponin and in-hospital mortality of COVID-19: an insight from a meta-analysis. J. Med. Virol. 93, 51–55 (2021). https://doi.org/10.1002/jmv.26108
5. Patone, M., Mei, X.W., Handunnetthi, L. et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat Med 28, 410–422 (2022). https://doi.org/10.1038/s41591-021-01630-0
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








