
People who discuss the US mortality event of spring 2020 in a serious, intellectually honest way generally acknowledge that at least some Americans were killed by human interventions — especially misuse of mechanical ventilators, and especially in New York City.
Along those lines, Michael Senger posted a good summary this week of the early clamor over and (mis)use of mechanical ventilators, with estimates of how many April 2020 deaths are miscoded as covid deaths that should be coded as vent-expedited or other iatrogenic deaths.
Due to my ongoing interest in New York City’s nonsensical spring 2020 death toll, Senger’s estimate for NYC caught my eye. He says 17,289 of the city’s April 2020 excess deaths may be from vent (mis)use and other interventions. (Note that Michael Senger uses a weekly excess death data file from CDC – whereas I am using monthly 2020 numbers from CDC Wonder.) CDC WONDER’s Place of Death (There are 8 categories of “Place” in US morality data: healthcare – inpatient, healthcare – outpatient/emergency department, dead on arrival, decedent’s home, hospice facility, nursing home/long-term care facility, other, and unknown. The numbers for DOA and unknown are very small.) stats provide a good “check” on this number.
Spring 2020: Where NYC Residents Died
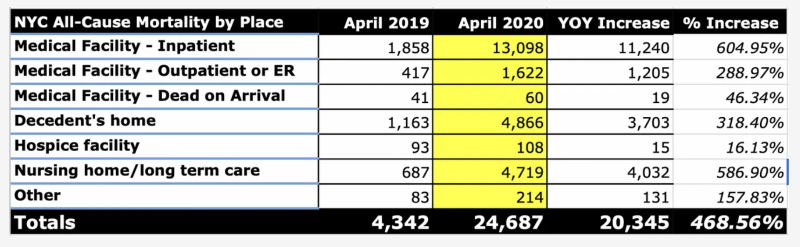
Here’s NYC all-cause mortality by place of death for February through May, 2020, followed by all-cause mortality comparison between April 2019 and 2020. (I say “increase” rather than “excess. “Excess” is based on predictions from a statistical model, i.e., how many *more* occurred than what the model expected, based on factors such population growth, age groups expanding and aging, etc. “Increase” is simply how many more occurred than the comparative time frame. We would expect some increase between April 2019 and April 2020 simply as a function of time. So, not all increase should be viewed as unexpected or “excess.”)
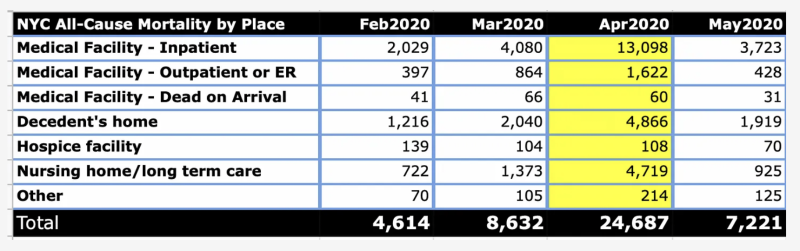
With over 20,000 (!) more deaths in April 2020 than in April 2019, Senger is right to assert that non naturally-occurring factors were at play, and wonder how many deaths those factors account for.
Potential Vent Deaths
Re: vent-assisted deaths per se (versus panic, neglect, healthcare-avoidance and other policy-related causes), we can effectively rule out decedent’s home, hospice facilities, dead on arrival, and other as places such deaths would’ve happened. Together, those comprise 3,868 of the YOY increase, which brings the 20,345 increase down to 16,477 — 812 deaths fewer than Senger’s estimate for iatrogenic deaths. That 16K+ took occurred in hospitals, outpatient facilities/ERs, and nursing homes.
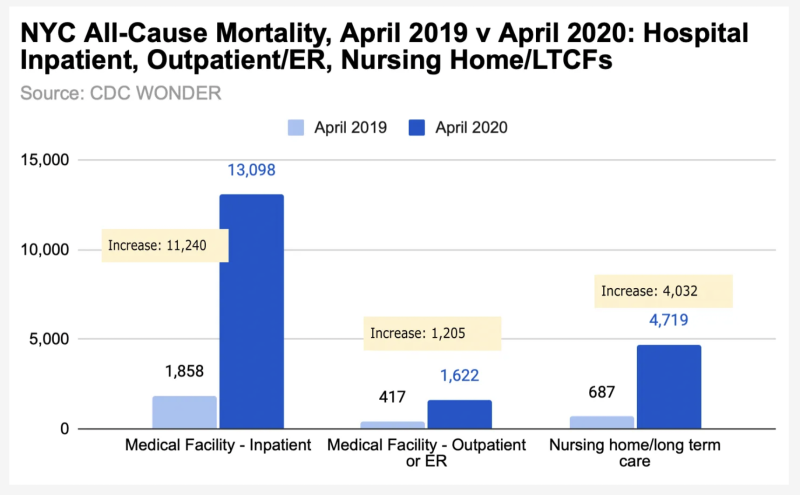
As far as I know, the emergency vent supply was sent mostly to hospitals, not nursing homes, where they were pushed as a necessary life-saving measure.
Senger assumes — and I agree — that vent-expedited deaths would have been attributed to covid. The proportion of deaths at each of these types of place that did and didn’t have covid on the death certificate is shown below. The 13,937 total is 3,352 lower than Senger’s estimate for iatrogenic deaths.
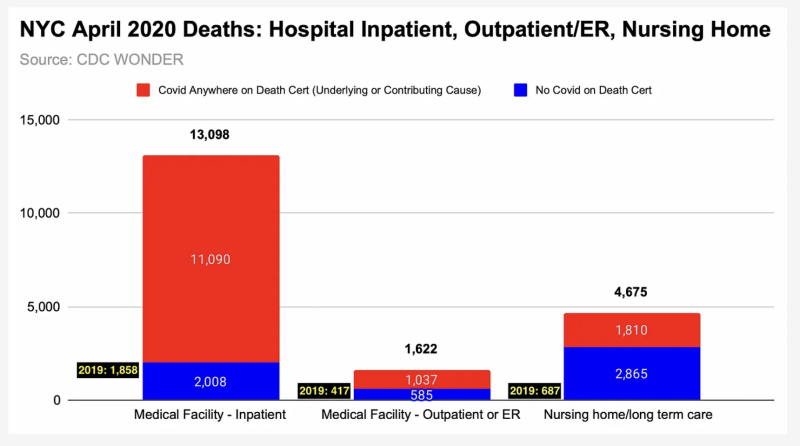
Given the length of time covid+ patients were intubated, hospital inpatient (which includes ICU) data was more likely than the ER or an outpatient facility to include Covid+ patients who were placed on mechanical ventilators. It’s unlikely that all ~11K of those deaths were patients placed on ventilators. (It would be nice for CDC WONDER to add that reporting criterion, so we could know for sure.)
Some are simply covid+ deaths of people who were never on a vent – and people who were but for whom the ventilator legitimately didn’t play a role in their death.
How many people were in those groups is hard to say — and other iatrogenic factors absolutely could’ve played a role in most April 2020 “excess” deaths that occurred in NYC’s healthcare/nursing home facilities. But it seems the city’s death-by-vent number per se is no higher than 10,000.
Back to Senger’s Estimate
Vents aside, Michael Senger’s 17K+ seems like a solid estimate for the number of NYC residents who died in April 2020 as a direct or indirect result of the government’s response to covid, versus covid itself.
To illustrate, here’s NYC Place of Death for that month again, with deaths that attributed covid as underlying cause (versus covid as underlying or contributing cause).
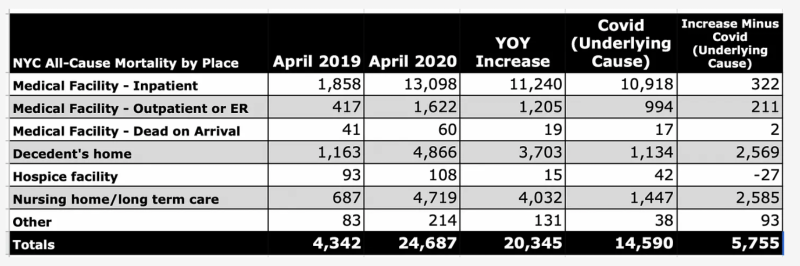
Almost 6,000 deaths aren’t being passed off as caused primarily by the virus. What would those covid-as-underlying-cause numbers look like with an honest covid case/death definition? The 1,134 alleged covid deaths at home is highly suspect on its face, save for some folks who may have been in a hospital or nursing home (on a vent?) and then died at home. Limiting covid deaths to those who were actually experiencing respiratory distress, for example, would likely reduce the healthcare and nursing home numbers by 50% or more.
Some other observations…
Covid is on the death certificates of nearly everyone “above” the increase (vs 2019) in NYC’s April 2020 hospital inpatient deaths. Does that make sense? Only when we consider the sociological/psychological influence that financial incentives that hospitals and survivors of the deceased have received. Lots of attention has been on the city’s nursing homes during this timeframe, but where is the audit of these hospital numbers?
Speaking of nursing homes, of the 4,032 increase in April 2020 deaths (vs April 2019), less than half had covid on the death certificate. Maybe these are part of the “presumed” in-facility deaths that New York is counting in its state toll? (The CDC and NY numbers on that score don’t jibe, as I explained in this post.) Some residents died from/with covid in hospitals (on vents?) – around 2,100, if NY state’s data is correct.
Further investigation and study is needed to determine which factors contributed to resident deaths, covid+ and otherwise. I suspect the virus — and Cuomo’s directive that said nursing homes shouldn’t turn away admissions based on a patient’s covid status – is being unintentionally scapegoated to some extent, i.e., blamed for deaths that were actually due to withholding treatment, neglect, cutting off visitors, isolation protocols, etc.
Do Not Forget
Do not forget, dear readers: There was no discernible excess death in NYC prior to lockdown orders. We are supposed to believe covid was spreading silently, minding its own business, without necessitating more ventilators (or PPE or PCR tests) until elected & public health officials gave it permission to super-spread everywhere at once, triggering profitable – and wasteful – supply/demand opportunities. Even if attendant-mediated transmission played a role, it would mean the actions taken in the name of stopping a virus (one that was already here and circulating for many months) are the things that made it worse.
April 2020 was “the cruellest month” indeed. (Eliot used the British spelling for cruellest. I used the American English spelling in my headline.) May more analysis from Michael Senger and others help us figure out why, so that it never happens again.
Reprinted from the author’s Substack
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








