International public health operates around a clear set of dogmas, protected by maintaining taboos on discussion of subjects that might undermine them. This may seem backward or even alarming, but it is entirely logical. For a quarter century, the industry has been dominated by private investors and corporate interests who are attracted to a market for which products can be coerced and mandated without restrictive advertising standards. The growing narrative around climate and health promises to be the apogee of this approach.
Taboos and Dogmas
Human societies always maintain taboos. Some seem to have arisen by common consent, and some are driven from above, but it can be hard to identify their origins. Do cultural taboos on pre-marital sex or homosexuality, for instance, originally arise from the bulk of the population, or as restrictions imposed by religious or political authorities? Did a requirement to acknowledge the earth as the center of the universe reflect popular sentiment, or drive popular sentiment? Did the Inquisition in Europe grow through popular prejudice, or was it purely an organ of authoritarian control?
The Enlightenment supposedly brought Europe out of the Inquisition, and while true in some ways, it is also an illusion. Safe Spaces on university campuses are areas where the Inquisition yet lives. So are the protests against drag queen book readings, and the protests against the protests against drag queen book readings. We don’t need to think an Inquisition is right or wrong, just acknowledge that we all put limits on freedom of expression and filter which ideas can be shared.
Taboos, by their nature, impose blanket limits on freedom of expression. They require that the dogma they protect must be viewed as immutably true. This is why, though they are convenient, they are nearly always a bad idea. The world as we perceive it is nearly always full of exceptions to any rule we come up with. For example, we can hold that limits on free speech should be taboo, or always unacceptable. But this would require us to support the right of an adult to teach a three-year-old child how to commit murder or torture.
We may consider abortion is always wrong because it is never acceptable to kill an innocent child, but then support the bombing of a country that is trying to invade, rape, and pillage another. Our taboos and the dogmas that accompany them rarely stand the test of life. They require us to blind ourselves and so are anathema to the scientific method. However, they are vital tools for mass marketing if one must break a scientific approach in order to sell a product.
The Public Health Climate Inquisition
Public health professionals see themselves as Children of the Enlightenment rather than Children of the Inquisition. We claim the side of common sense rather than taboos and dogma. We think this sets us aside from the general public, which is easily persuaded through ignorance to entertain the rantings of charlatans.
Because we are educated and progressive, and health is so important, we claim a right to bypass much of the conversation that Enlightenment normally requires. We need to fast-track things to the truth because they are so important, and we are so knowledgeable about them. While this may seem reflective of the inquisitors of old, we hold that there is a fundamental difference; they were wrong, and we are right. Comparisons therefore simply show the ignorance of the accuser, whom we then label far-right or otherwise reality-denying. Climate change and its effect on health is a good example. This will become clear by explaining the official public health industry position in this area, which is critical both to continued human existence and to securing future funding.
Exchanging Truth for Permissible Narratives
The public health professions, not least at the international level, are adamant that climate change is an “existential threat.” Dogma states that this is almost solely driven by human activity, particularly the burning of the fossil fuels on which the last few hundred years of technological and medical progress have relied. It also implicates traditional meat diets in driving the climate. The Director-General of the World Health Organization is adamant that this must be his organization’s priority.
Two hundred medical journals considered it so important that they abrogated editorial standards to publish a letter highlighting various controversial claims as dogma; as an example a rapid increase in elderly deaths due to heat that ignored the simple increase in the total elderly population that accounted for most of this change, whilst far more die of cold. They were not ignorant of this – they just considered the issue so important that it was worth misleading the public in order to gain a required response.
So, this is where we are on climate in the public health sphere. We are funded, as a group, to impose someone’s dogma. “The Science is settled.” We are still all in favor of human rights and evidence-based policy, but we consider ourselves entitled to ignore them in order to protect them.
To explain further, it is useful to list what is deemed acceptable in the international public health industry to secure a salary and serve our funders:
- The climate is warming, and this will have overwhelmingly negative consequences on health.
- Human activity – particularly the burning of fossil fuels and farming for meat – are the primary drivers of climate change through CO2 emissions and emissions of nitrous oxide, methane and other greenhouse gases.
- If we don’t reduce emissions (reach net zero), we will face mass human death and potentially extinction.
- A warming climate is increasing pandemic risk.
- A warming climate is increasing extreme weather events, with a rising impact on health.
- Warm days, though common where most people live, pose an extreme threat to health.
- Climate change is driving increased malaria (see later), increased tuberculosis (previously thought due to poverty), and infectious diseases generally (irrespective of their continued overall decline).
- A warming climate could raise sea levels and enlarge deserts, destroying human settlements and agricultural land, and causing mass starvation and forced migration.
Some of these are true, or at least have a kernel of truth – although actual outcomes obviously depend on our ingenuity to cope with change, which we are historically very good at. Taken alone, this list constitutes a compelling reason to reach net-zero carbon emissions and force a change in diets. A delay through continued open debate would make outcomes worse. As a result, we have formed them into dogma and enforce this, protected by a series of taboos, including the following (which, to protect public safety, you can delete later):
- Climates changed frequently in the past (e.g. Medieval warm period, Roman warm period, 6,000 years ago (tree line further north near the Arctic Ocean) etc., and these were not driven by anthropogenic CO2.
- Reported acute infectious disease outbreaks have been decreasing over the past decade rather than increasing.
- Mortality from acute weather events has plummeted over the past century.
- Rising CO2 has increased global plant growth, which is a contributor to our ability to feed eight billion people, a feat many considered impossible.
- A warmer climate will likely extend productive agriculture in cool temperate regions such as Eurasia and North America, increasing food availability.
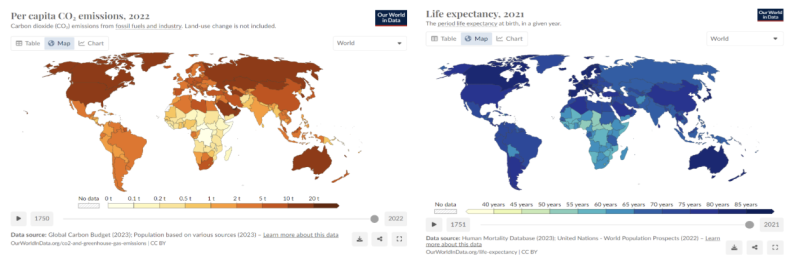
- The main driver of infectious disease and shorter life expectancy in low-income countries is poverty. The reason Western people live longer is because they became richer, and this happened primarily through the burning of fossil fuels – coal, oil, and gas – in industry, transport, farming, construction, sanitation, and in the manufacture of fertilizer and medicines. Wealthy countries still burn many-fold higher volumes of fossil fuels per person, and correspondingly release more CO2, than poorer countries where people live much shorter lives (see graphic).
- Over three billion people still rely on wood-based cooking (or burning dung) and this is a major cause of deforestation and regional climate change and desertification (e.g. in East Africa), indoor air pollution (that contributes to over a million deaths per year), and impoverishment and physical risk for women (who must walk miles to collect wood).
- China and India are rapidly increasing their coal-burning capacity and CO2 outputs to achieve the benefits that wealthier nations have, and this will far outweigh CO2 reductions achieved in the West or forced on other poorer and less powerful countries.
This second list is demonstrably true. But such is our concern and discipline (we prefer these terms to ‘fear’ and ‘cowardice’) that we don’t discuss them in open forums. Even poverty reduction, once integral to public health, is now taboo in the context of climate change. Public acknowledgement that net-zero policies entrench poverty and inequality would put the entire narrative at risk.
Malaria as an Example of a False Example
Malaria is interesting as it exemplifies public health’s move to dogma over debate. I have been in forums of malaria ‘experts’ where they agree in small groups that there is little compelling evidence associating climate change with worsening malaria, but in a subsequent plenary none will question this claim. I have been pushed to falsely implicate climate in a report for a major international health agency as a driver of worsening malaria, though it was agreed the evidence on which the report was based did not support this. As a profession, lying is deemed acceptable if the subject is important enough. One agency claiming this justifies another to highlight it, which can then be used as evidence of consensus by the first. More funding all round.
It was popular 15 years ago to call malaria “a disease of poverty.” It is. It also requires a warm moist environment to support the mosquito vector. Warmth improves mosquito survival and, importantly, reduces the time taken for the parasite to mature in the mosquito before it can infect another human. However, malaria is no longer endemic in Singapore and is now rare in Malaysia, because they have become wealthy. Money allows access to insecticide-treated bed nets, diagnostics, medicines, and good supply lines, which stop malaria. However, it still kills over half a million children every year.
Malaria has indeed spread in the highlands of Papua New Guinea and Ethiopia, as a warming climate allows mosquitoes to live at higher altitudes. However, countries further from the Equator that should be most impacted by a warming climate allowing mosquito habitats to move north and south are seeing the greatest progress in malaria elimination.
On a global scale, malaria mortality has risen since early 2020, with progress having slowed or reversed some years earlier. There are many contributors to this. We have growing resistance to the insecticides used in bed nets and house spraying (alternatives are more expensive), some increasing resistance to major antimalarial medicines, and genetic changes in the parasite that have made it harder for some blood tests to detect them. A diversion of human resources occurred from malaria programs to (demonstrably pointless) Covid-19 vaccination programs. There is also a reduction in funding in real terms, and an increasing funding gap to provide access to the core interventions – nets, spraying, diagnostics, and drugs – that malariologists consider essential, whilst at-risk populations increase due to high birth rates.
This complexity is becoming harder to discuss. Now, climate change is proclaimed the major threat to health, soon to “overwhelm the world’s health systems,” and the WHO and partners are prioritizing reaching net zero. It is not that climate change is irrelevant to malaria, but that the malaria community is unable to actually weigh it, and proposals for its mitigation, in an objective manner. Net-zero policies will logically exacerbate poverty, increase transport costs, increase malnutrition, and thereby drive higher overall malaria mortality, but such discussion is taboo.
We Can Choose Slavery or Science
So, the issue of health, climate, and CO2 is complicated. One way to cope with complexity is to ignore it. The WHO now adopts this approach, and literally invents a narrative, maintaining that “…ever-increasing climate-mediated disasters create humanitarian emergencies where infectious diseases can take hold and quickly spread.” This creates media headlines but loses the trust of rational people once they are exposed to reality.
A rational assessment may even conclude that, through increasing the human food supply, rising CO2 and perhaps even warmer temperatures may provide an overall health benefit. Or, they might be outweighed by negatives, which are real in many regions. Some areas will lose rainfall, some may see more floods, and if the sea level rose by 20 feet it would create a crisis the likes of which we have not seen in history. But stopping this would depend on the current global warming episode being almost entirely due to human action while those in the past were not (interesting) and then these causes being remediable without causing net harm to over 8 billion of us, which is highly unclear.
In public health, we do not discuss this, as it is awkward. We maintain this taboo for one of two reasons:
- The consequences of a warming climate are so dire that the risk is not worth taking. We therefore consider that a relative few of us in wealthy countries have the self-assumed right to impose our solutions on the rest of humanity, keeping them in poverty while we thrive.
Or,
- Wealthy donors, with influence over public health priorities and important investments in climate change-related technologies, expect us to do so. Our job includes selling their product.
The first reason is essentially fascist, whilst the second is cowardice. Either way, we are acting falsely and disingenuously about climate change and health, and we all know it. We label the second list of bullets above as misinformation and censor it. If we argue that we are doing this for a greater good, we therefore see this within the hierarchical, feudalist model that allows a few to dictate restrictions and poverty on the many. We have chosen the side of the Inquisition, not the Enlightenment.
Alternatively, we could embrace the truth, however dangerous and worrisome, through a rational and open discussion. Rather than throwing abuse and derogatory remarks at those who hold a different line, we could examine our own position and weigh it against theirs.
This might help restore trust in public health, but it could also wreck our careers. It all comes down to where we place ourselves, and others, in a hierarchy of values. We can play it safe and be slaves to an Inquisition that oppresses and impoverishes the many, but benefits a few including ourselves. Or we can risk following the truth wherever it may lead. But that, in the current climate, would take courage.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








