
1 – Stirring the Pot
On February 3, 2023, the New York Times ran an opinion piece by Zeynep Tufekci titled, “An Even Deadlier Pandemic Could Soon Be Here.”
Here is the nutshell version of her article: Avian flu has been around for years and “hasn’t often infected humans,” but the H5N1 strain (which has been in circulation since 2014) could become deadly dangerous, so we need lots of testing, new mRNA shots, and global surveillance – right now! Ramp up the testing! Increase the government’s H5N1 stockpile! “Mass vaccination of poultry and pigs should begin quickly!” along with “voluntary vaccination”…of “poultry workers and health care workers.”
Tufekci is a sociologist, a professor at Columbia University’s Craig Newmark Center for Journalism Ethics and Security, and a faculty associate at Harvard’s Berkman Klein Center for Internet and Society. What Tufekci is not, is a medical doctor, scientist, biologist, vaccinologist, epidemiologist, disease expert, or public health expert.
To be fair, as Dr. Scott Atlas states, “You don’t have to be a medical scientist to understand the data. You just have to be a critical thinker.” However, we must fault Tufekci on both counts – the data and critical thinking. In what can only be considered a hit piece on the world, Tufekci makes broad scientific and medical claims about viruses, citing inaccurate data and making mostly vague references to “experts.”
Tufekci writes, “The world needs to act now, before H5N1 has any chance of becoming a devastating pandemic.” She cites a 56 percent fatality rate in those who have contracted H5N1. Apparently she is referring to a January 2023 World Health Organization publication that reports 870 cases of bird flu in humans over the past 20 years, of which 457 were fatal. Stop and think about that for a minute. The most significant part of the WHO report is not the more than 50 percent mortality rate, but that the data spans 20 years. As the WHO report states, “The likelihood of sustained human-to-human transmission of these viruses remains low.”
In an avian flu article updated January 27, 2023, the CDC reports that fewer than 10 cases of humans infected with H5N1 bird flu virus have been reported globally since December 2021. The CDC notes that H5N1 is “primarily an animal health issue,” and explains, “Human infections with bird flu viruses have most often occurred after close or lengthy unprotected contact with infected birds.” The CDC states, “The spread of bird flu viruses from one infected person to a close contact is very rare, and when it has happened, it has not led to continued spread among people.”
But it appears someone wants the public to panic.
On February 8, 2023, just five days after Tufekci’s article was published, the WHO’s director-general Tedros Adhanom Ghebreyesus warned that, because the H5N1 has jumped from birds to mammals, “the world must prepare for a potential human bird flu pandemic.” Did Tufekci and The Times get a heads up? It’s hard to say, but on the day of the WHO’s press conference, the Daily Mail in the UK wrote an article quite similar to Tufekci’s opinion piece. It would appear both writers got their talking points from the same source, which would mean there wasn’t a lot of objective investigative journalism going on.
The WHO, the NY Times, and the Daily Mail all mention that avian flu H5N1 does not infect humans easily, or other mammals, but also state that the spread of bird flu poses a possible global risk until brought “under control.” Of note, there is an average of 56 million deaths worldwide per year, due to all causes; in a three-year period, Covid-19 has killed just under 7 million people. Comparably, the Spanish flu of 1918 killed 50 million people, which would amount to upwards of 219 million people if adjusted for today’s population.
Covid-19 itself, has not been remarkable for its high death toll in those under age 60, although it’s a much more serious disease for the elderly, and those with comorbidities, as are all respiratory illnesses.
2 – The unscientific response to Covid-19
What has been remarkable, and terribly disturbing, was our unscientific response to Covid-19. It’s as if 100+ years of medicine and social science were simply wiped out – no understanding of natural immunity, failure to treat the various symptoms of Covid, failure to acknowledge the stratified age risk, no recollection of the nature of coronaviruses, no knowledge of how to treat pneumonia or reduce the risk of blood clots, no memory of how to handle busy flu and cold seasons, no reference to carefully laid out prior pandemic planning, complete disregard for the need of hospital patients and residents of care centers to have loved ones with them to foster better healing and health, callous indifference to the harms face masks and school closures would surely cause children. All was forgotten or cast aside.
Will we do the same with H5N1, or some other pathogen? Although H5N1 first emerged in 1996, and has never spread widely to humans, the fact that in the past year or so it has also begun infecting mammals is concerning. Yes, but not as concerning as Tedros saying it’s concerning, based on how the WHO has handled recent virus outbreaks.
Remember Monkeypox last year? In July 2022 the WHO declared it a global health emergency, based on a few thousand cases worldwide, leading the US to also declare Monkeypox a public health emergency on August 4, 2022. As CBS News reported at the time, the emergency declaration “could unlock a broad swath of flexibilities in funding and regulations to respond to the spread of Monkeypox…” and “would allow the Food and Drug Administration emergency use authorizations that could ease access to treatments and vaccines for the Monkeypox outbreak.”
We’ve seen a lot of “funding and regulations” during Covid, and it wasn’t pretty. “Easing access to treatments and vaccines” means rushing new products to market. Indeed, the bivalent booster for Covid-19 was deemed so urgent that there was “no time” for human trials; it was only tested on eight mice before being approved for worldwide human use, including for children and infants.
3 – What vaccines do, and don’t do
Where did this idea that vaccines are the answer to every illness come from? How is it that the amazingly complex human immune system, and its ability to fight diseases, is ignored these days in discussions about viruses?
Here are some truths about vaccines from a knowledgeable individual who writes under the pseudonym El Gato Malo:
- “A vaccine cannot teach you to do something that you could not otherwise do. It’s just intended to be a safe way to…teach you to resist infection without running the risk of getting infected.”
- “ALL the vaccines that really do stop you from contracting and spreading diseases have one thing in common: they work on a ‘one and done’ virus that does not mutate. Measles, smallpox, chicken pox, mumps, rubella, these are all diseases where you get them once and…you never get them again.”
- And now, a most important truth: “There has never been a successful vaccine for a recurrent respiratory disease. Not for flu, coronaviruses, RSV, none of it. These viruses mutate too quickly. There is always a new one, a new strain, and it will infect you whether or not you got sick last year.”
- “mRNA vaccines are about the worst possible way to go about this as they do not even teach your body to recognize the virus itself, only the effects in infected cells.”
That is, mRNA shots teach your cells to make the spike protein, which is only one of 29 proteins that make up the SARS-CoV-2 virus. Unlike someone with natural immunity, a vaccinated person’s body has not learned to fight SARS-CoV-2, but only to attack the spike protein. And devastatingly, the mRNA Covid-shot turns the human body into a spike protein factory, causing self to attack self.
Ramping up mRNA production, and increasingly administering shots to the general population, is not going to eliminate the common cold, Covid-19, influenza, or RSV. Barring a compromised immune system, due to age or other comorbidities, the body’s own immune system is perfectly capable of handling the return of cold and flu season each year, of which Covid-19 is now a part.
4 – Undermining the body’s immune system
Human beings live in an environment of viruses and bacteria, and have done since the beginning of time. In today’s interconnected world, we all are exposed to the same viruses; there will not be a repeat of wiping out whole populations due to being virus naïve, as happened in the Americas when the Conquistadors showed up. There will not be a repeat of the 1918 Spanish flu that occurred in the early days of modern medicine, before the discovery of antibiotics and the development of effective treatments for all types of medical conditions.
Dr. Shucharit Bhakdi, who spent his career as a researcher and professor in the field of medical microbiology, infectious disease, and immunology makes an insightful point that, “There is no such thing as a medical emergency nowadays because modern medicine has come such a long way, and the doctors around the world are good enough to take care of anything.”
Dr. Geert Vanden Bosche, a vaccinologist and virologist stated in a 2021 interview, “The whole mistake in this pandemic is the complete neglect [of] the incredibly important role of the innate immune system to defend against the virus.” He explains why the mechanism of the mRNA shots is so dangerous to the natural immune system, especially in the case of children, whose developing immune system can actually be permanently derailed by the mRNA shots. Data coming in from various studies are showing that the more Covid shots a person receives, the more susceptible they are to Covid.
The Cleveland Clinic study, involving 51,000 participants, analyzed incidents of Covid-19 infection in employees from September 12, 2022 to December 12, 2022. (September 12 was the day the bivalent boosters became available.) The study found that the “bivalent COVID-19 booster was 30% effective in preventing infection, during the time when the virus strains dominant in the community were represented in the vaccine.” (The bivalent shots targeted the original Wuhan strain which was no longer circulating, and the Omicron variant, which is rapidly being replaced by the BQ and XBB variants.)
One finding in the study was, “The more recent the last prior Covid-19 episode was the lower the risk of Covid-19, and that the greater the number of vaccine doses previously received the higher the risk of Covid-19,” as shown in the following chart:
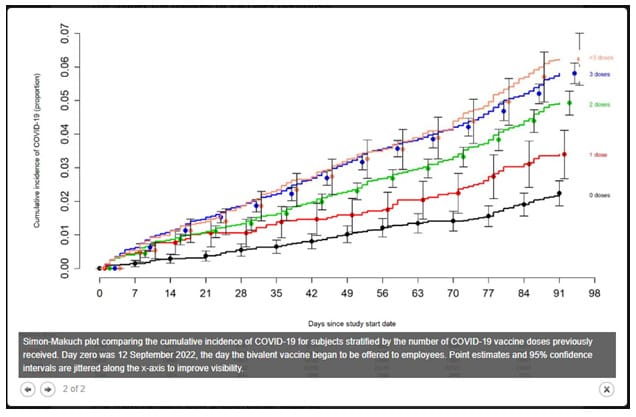
Although the study concluded that the bivalent booster gave a 30 percent protection against infection, the more telling finding is the correlation between the number of Covid shots and the likelihood of Covid infection. This finding ties in with the emerging concern that repeated exposure to the spike protein is activating IgG4 antibodies in the immune system.
Generally we think of increased antibodies as a good thing, but as writer Igor Chudov explains, “IgG4 antibodies have the opposite effects to all other types of antibodies and make our immune system ignore the particular antigen they are trained to detect.” That’s a good thing when it comes to allergies, but not when it comes to viruses. Chudov states, “Switching to IgG4 binding against a viral agent is like opening your house doors wide for robbers and ignoring them as they ruffle through your drawers. The robbery will be ‘mild’ – but the thieves will take away your stuff. And they will come back again.”
So why would natural immunity be downplayed or even ignored in connection with Covid-19 and the rollout of the Covid shots? One could surmise that there is no money to be made by acknowledging the strength of the innate immune system and natural immunity. The money is in drugs and vaccines.
5 -Follow the money
Without going into details here, an acknowledged truth is that multiple agencies within the US Department of Health and Human Services (HHS) are on the receiving end of millions of dollars from the pharmaceutical companies they supposedly regulate (see here, here, and here). Among the many divisions in HHA are the Food and Drug Administration (FDA), the Centers for Disease Control and Prevention (CDC), and the National Institutes of Health (NIH).
As Dr. Aaron Kheriaty, psychiatrist and medical ethics professor explains, “[M]ost people are still unaware that the NIAID, Fauci’s division (before he retired) of the NIH, owns half the patent on the Moderna vaccine, among thousands of other Pharma patents.” A non-profit group, Open the Books, used documents obtained through FOIA requests, to determine that 1,675 NIH scientists received combined royalties of up to $350 million from third parties during the fiscal years between 2010 and 2020. The documents showed that (former) NIH director Francis Collins received 14 payments, Dr. Anthony Fauci received 23 payments, and Fauci’s deputy, Clifford Lane, received eight. Tellingly, Dr. Fauci’s household net worth almost doubled during the pandemic, from $7.5 million in 2019 to $12.6 million at the end of 2021.
This type of money exchange between the regulators and the pharmaceutical companies leads to conflicts of interest that do not serve the public well. Tufekci’s piece ignores the financial incentives of continuous vaccine manufacturing and distribution, and is particularly troublesome in her call for widespread surveillance, testing, and vaccination in response to the avian flu. She also suggests that the World Health Organization “take the lead in expanding global vaccine manufacturing.” That is the last thing we need. There was a decidedly militant aspect to the official Covid-19 response, to which the WHO contributed.
6 – Pandemic response as a means of control
This May, the World Health Organization will again attempt ratification of changes to the International Health Regulations (IHR) treaty it has with member nations. The changes would authorize the WHO to declare a pandemic or epidemic in any country and mandate the course of action they must take. Last year the WHO’s attempt to pass similar legislation failed, largely because many African countries refused to sign away their sovereignty. The WHO, which is operated by unelected officials, is a useful organization for identifying disease trends and sharing global medical information, but has no business enforcing anything. Medical responses are best handled at local levels based on which areas and populations are at risk. Unfortunately the American people have the current presidential administration to thank for the suggested changes to the IHR.
As playwright and political satirist CJ Hopkins points out, the Covid-19 response introduced us to something never seen before on a worldwide scale: “revocation of basic rights and freedoms, centralization of power, rule by decree, oppressive policing of the population, demonization and persecution of a ‘scapegoat’ underclass, censorship, propaganda, etc.” Hopkins calls our current situation “New Normal totalitarianism,” and explains the insidious nature of “reality” being defined by authoritarians: “Those who challenge ‘reality’ are ‘insane,’ i.e., ‘conspiracy theorists,’ ‘anti-vaxxers,’ ‘Covid deniers,’ ‘extremists,’ etc.,” and effectively discredited and marginalized, if not silenced.
In his book The New Abnormal: The Rise of the Biomedical Security State, Dr. Aaron Kheriaty writes, “Public health’s gradual militarization is a decades old development, massively accelerated by the Covid pandemic.” (p. 37) Indeed during the past 20 years the government and corporate sectors have engaged in table top exercises – pandemic war games – simulating every detail of pandemic response from all angles, including how to handle the vaccine hesitant, and dissenters from the official narrative.
As outlined in a recent piece by investigative journalist Debbie Lerman, Covid-19 pandemic policy-making was not primarily headed up by US public health agencies, but by the National Security Council and the Department of Homeland Security. Lerman states, “[O]ur response to the Covid pandemic was led by groups and agencies that are in the business of responding to wars and terrorist threats, not public health crises or disease outbreaks.”
Lerman continues, “Furthermore, all of the seemingly nonsensical and unscientific policies – including mask mandates, mass testing and quarantines, using case counts to determine severity – were imposed in the service of the singular goal of fomenting fear in order to induce public acquiescence with the lockdown-until-vaccines policy.”
Dr. Kheriaty confirms this idea, when he explains, “Consistent themes [in the pandemic war games] included militarizing medicine and empowering centralized authoritarian governance capable of broad surveillance and behavioral control of large populations. Every one of these scenarios ended with coerced mass vaccination.” (p. 38) Crimson Contagion, a pandemic table-top exercise that was completed in August 2019, simulated in detail a respiratory virus outbreak that closely mirrors what happened just a few months later. In fact Robert Kadlec, a biodefense consultant and career US Air Force officer and physician, was the coordinator of Crimson Contagion, and became the assistant secretary for preparedness and response at the US Department of Health and Human Services during the Covid pandemic. Kadlec’s focus is on biodefense – not public health.
7 – Milking the narrative of “Emergency!”
The New York Times does not appear to be interested in spending much column space on analyzing the pros and cons of the official Covid response. It does appear to be interested in priming its readership for another pandemic. Interestingly, there was another Times Opinion piece in October 2022 about bird flu, with a headline like the start of a bad joke “A Dolphin, Two Porpoises, and Two Men got Bird Flu. That’s a Warning to the Rest of Us.”
The Covid-19 pandemic put in stark relief the troubling lack of investigative journalism in most mainstream media, perhaps largely because a large portion of their advertising dollars come from pharmaceutical companies. During the pandemic, prominent media outlets have often been in the business of “narrative,” rather than news. When a narrative is being pushed by media, it starts in the opinion pages and moves to the news columns. These two NY Times opinion pieces are indeed a warning, but not of a dangerous pandemic. Rather, they are evidence that the powers that have kept us in turmoil for the past three-plus years are planning to repeat the process.
American philosopher Matthew B. Crawford recently reflected on the Covid-19 pandemic as part of a broader topic: The Perpetual State of Emergency. Crawford explains that historically there have been crises – such as plague, foreign invasion, and natural disasters – that create a state of emergency, or “state of exception” in which the legislative function of a country is relocated from a parliamentary body to the executive, until the emergency passes.
Crawford continues, “The language of war is invoked to pursue ordinary domestic politics. In the U.S. in the last 60 years we’ve had the war on poverty, the war on drugs, the war on terror, the war on Covid, and now the war on disinformation, (and) the war on domestic extremism. So it becomes normalized to have a state of emergency.” Obviously the “climate emergency” can also be added to that list.
It seems for most of us that life goes on, somewhat normally, as emergencies are supposedly all around us. But what we don’t always perceive on the larger scale is the long-term loss of liberty that is at play – the fundamental shift from democracy to tyranny, due to continual declarations of emergency. For example, since March 2020 the US has been, and still officially is, in a state of “medical emergency,” during which time there has been a wide suspension of constitutional rights either in actual practice, or as an ever present legal threat. Surely this belies both the definition and intent of emergency powers. (Attorneys General from 16 states are suing the Federal government to end the state of emergency immediately – not on May 11, as Biden has proposed.)
Crawford states, “I think what’s made us acquiesce in this, is really propaganda, more than anything else. We saw a determination to control information with Covid that was radically anti-scientific. The science was getting settled, so called, not by the usual process of science, but through intimidation and policing of hypotheses and efforts to make sense of it all…I think there’s a patently desperate effort to control discourse and information so as to not interrupt the…machinery of emergency politics.”
8 – Ignoring reality and promoting propaganda
I would define the two NY Times opinion pieces referred to in this article as propaganda. Tufekci’s article is full of errors; for example she overstates the infection fatality rate (IFR) of Covid-19 by magnitudes, saying Covid “is estimated to have killed 1 percent to 2 percent of those infected before vaccines or treatments were available.” In the most recent meta-analysis conducted by John Ioannidis and colleagues of the Meta-Research Innovation Center at Stanford University, the data showed the global IFR for Covid-19 was 0.03 percent before the vaccine, in the 0-59 age groups. The IFR is higher for the elderly, but still well below the 1 percent Tufekci sites.
Even back in 2020, when much less data was available, Ioannidis determined the IFR for young people was in the range of 0.20 percent and for the elderly it was closer to 0.57 percent. There is no excuse for Tufekci, or the NY Times editors, to make such an egregious error in an article that purports to be presenting views based on biology and virology. Perhaps of most concern is Tufekci’s enthusiasm for expanding the mRNA platform to make influenza shots.
Tufekci is either unaware, or does not want to acknowledge, the evidence the mRNA technology needs much more research and refinement before being used in vaccinations. The mRNA Covid shots, which were neither properly vetted nor administered to people with informed consent, have injured many, but especially young people.
Life insurance companies report that starting in the third quarter of 2021, there was a 40 percent increase in death rates, with the biggest increase in working-age people 18-64. Life insurance CEO’s point out that the deaths were not due to Covid. Most startlingly, it’s the highest increase in excess mortality ever seen in the history of life insurance. In addition, the companies have seen an uptick in disability claims.
Edward Dowd, former Wall Street analyst and Managing Director of for BlackRock, has analyzed the excess mortality reported by life insurance companies, in his book Cause Unknown: The Epidemic of Sudden Deaths in 2021 & 2022, Dowd presents this chart from the Group Life Covid-19 Mortality Survey Report of the Society of Actuaries Research Institute (SOA):

Note the increase in excess mortality in Quarter 3 of 2021, and which age groups were most affected. Dowd states, “Obviously this evidence is very compelling that something new and novel was happening to insured, working employees in 2021 that did not happen in the years prior to 2020 when COVID was raging.
“Using rudimentary deductive reasoning there is only one thing changed in 2021 and it wasn’t the virus, which was becoming less virulent. The employed insured population was forced to take an experimental vaccine product to maintain their employment—even if they were hesitant, or had a medical or religious objection—while those who were unemployed or retired had a choice.” ~ Dowd, Ed. Cause Unknown: The Epidemic of Sudden Deaths in 2021 & 2022 (Children’s Health Defense) (p. 344). Skyhorse. Kindle Edition.
Some are quick to point to other possibilities for the increase in excess mortality, such as drug overdoses, suicides, and delayed diagnosis of other diseases. Dowd explains that it is statistically impossible “for deaths to spike in any or all of the proposed categories within that exact same time period…there is no other factor (besides mass vaccination) that affected nearly all working-age people simultaneously.” In addition, the excess death rate is 8 percent higher in working-age Americans than in the general population, even though the general population is “far less healthy than working Americans.”
9 – Warning voices
Accounts are pouring in daily of Covid vaccine injuries, and deaths in athletes, young people, airline pilots, military personnel, and the general population. The failure of the government to stop the Covid vaccination campaign, and investigate further, is both grossly negligent and shocking, and speaks volumes to their lack of real concern for the people they are tasked to protect.
Evolutionary biologist Bret Weinstein states that officials tried to “strong-arm a consensus” about how to handle Covid-19, but that we should not expect a consensus in the face of an emergency like this that is so complex and has so many facets that are not well understood. He says doctors should have been left to their own devices, treating patients and exchanging information about what worked, and what didn’t, and the picture of how to address Covid-19 would have emerged naturally from clinicians. “Instead,” Weinstein says, “It was handed down; it was preordained. And that is completely unnatural; it was extremely dangerous, [and] it resulted in a serious violation of the Nuremberg Code.” Weinstein believes that not only has the Covid-19 response caused large-scale harm, but it has also led to a reduction in human longevity.
Cardiologist Dr. Peter McCullough stated In June 2022, “The mRNA vaccines (Pfizer, Moderna) and adenovirus vaccines (J&J, AstraZeneca) obviously don’t work; they don’t stop Covid-19 – neither the initial case nor do they stop transmission, and the vaccines unfortunately have a catastrophic effect on safety – the risk of death, serious non-fatal injuries and disabilities…This has been, in a sense, the crime of our lifetime, if not of all time – a mass vaccination of the world in the middle of a highly prevalent and evolving pandemic.”
Nobel Prize in Medicine winner Luc Montagnier warned in May 2021 that mass vaccination into the population in the midst of the pandemic was “unthinkable” because it would create super variants, and would lead to more chronic diseases and deaths.
Dr. Robert Malone, a pioneer in mRNA technology states, “It is grossly naïve…to believe that we have such a sophisticated understanding of virology and immunology and viral evolution that we can predict and administer something like this into the whole population and mitigate the natural process and come up with something that’s better than what has naturally evolved over millennia.”
Dr. Aseem Malhotra, a prominent cardiologist in the UK, was one of the first people to receive the Covid-19 vaccine and was a public advocate for the vaccine campaign. He has since become an outspoken voice for stopping the shots, stating, “It is my duty and responsibility as a consultant cardiologist and public health campaigner to urgently inform…that the Covid mRNA vaccine has likely played a significant role of being a primary cause of unexpected cardiac arrests, heart attacks, strokes, cardiac arrhythmias and heart failure…until proven otherwise.”
Conclusion: Rinse and Repeat versus Throw it Out and Start Over
Dr. Fauci, proponent extraordinaire of the Covid-19 shots (and lockdowns and masks) was one of the authors of a paper released in January 2023 that includes this query: “If natural mucosal respiratory virus infections (e.g. Covid-19, influenza, RSV) do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines…to do so?”
That’s a really good question Dr. Fauci. Would that you had asked it, and answered truthfully, before participating in the development, rollout, and mandating of experimental Covid shots that have caused the deaths of many people, and have negatively impacted the health of millions of others.
The question for the rest of us is this: Are we going to allow a repeat of what happened during Covid-19, or are we going to exercise critical thinking and our rights as citizens, to put an end to the growing biomedical security state? I choose the latter. We can start by critically examining what we’re being fed by the mainstream media, and by compromised government and public health officials, and refusing to be frightened and manipulated into another overreactive, unconstitutional, disastrous response to a pathogen.
Republished from the author’s Substack
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








