
During my weekend shopping in Melbourne, Australia, I was turned away from my favourite café and not allowed to sit even at an outside table by order of my master, the Chief Health Officer of Victoria. Later, I was told off for recklessly entering a food store to order a takeaway burger and muffin, a food store which I was allowed to enter last week but not this week.
Apparently, I might have been touching surfaces (I wasn’t, and Covid is not transmitted via surfaces). And then I blundered into the bakery, forgetting that only two people are allowed in at a time. Any business owner who might be confused by the fast-changing rules can consult the 47 pages of detailed formulations in the Chief Health Officer’s ‘Open Premises Directions (No 2)’ or seek help from their legal advisor. They are supposed to station a ‘Covid Marshal’ at each entrance of the premises to turn away the infidel (but this is not happening).
None of this obsessive micromanagement will make any difference to the course of the pandemic, but it puts relentless pressure on us all to get vaccinated, contributing to the State Government’s targets. It will declare victory over the pandemic when these targets are met and case numbers go down over the summer. Next August they may well go up again, and there will be renewed pressure to lock us all up, vaccinated or not.
I was denied entry to these premises because I am one of the unclean, yet to be vaccinated, and so a danger to public health (even more so than last week, apparently). Worse still, I have a subversive tendency to think for myself and like to make my own decisions about everyday activities and health strategies. Under new pandemic laws introduced into the State legislature this week I could be sent to jail for two years for disobeying a health order.
Of all the unprecedented violations of human rights and individual liberty that have been inflicted on populations during the Covid-19 pandemic, the most intrusive has been the relentless campaign to coerce every last individual to be vaccinated.
In the first phase of the pandemic, experts scared the hell out of governments with the unverifiable claim that staggering numbers of people would die if they didn’t try to suppress the circulation of the virus (by suppressing the circulation of the whole population) over a period of eighteen months or more ‘until a vaccine became available.’
Now that vaccines have become available, governments are pivoting from mass suppression of mobility to mass vaccination. Both strategies assumed that only universal methods would succeed. Both are driven by a wildly exaggerated and disproportionate view of the risks posed by Covid-19. Over one in five US adults believe that the risk of hospitalisation is 50% according to a Gallup survey, whereas it is actually less than 1% for most of the population. Governments should know better but they don’t.
And one of the most prominent distinguishing features of this pandemic is that risk (of severe illness and death) is heavily concentrated in the top two quartiles by age. Covid risk increases exponentially by age, as David Spiegelhalter has explained. Levin et al came to the same conclusion, and calculated infection fatality rates (IFR) for the different ages:
The estimated age-specific IFR is very low for children and younger adults (e.g., 0.002% at age 10 and 0.01% at age 25) but increases progressively to 0.4% at age 55, 1.4% at age 65, 4.6% at age 75, and 15% at age 85.
We can clearly see here that there is a watershed just before age 65 at which the IFR exceeds one per cent.
Universal strategies are rarely successful. Indeed, they hardly qualify as strategies at all, as the whole point of strategy is to concentrate resources on the problem at hand, which in this case was the intense vulnerability of the elderly. Strategy involves making choices, not trying to cover everything.
Instead of concentrating their resources on protecting the vulnerable, governments chose to try and control every organisation and every individual in an undiscriminating and undifferentiated way. Whereas the eminent authors of the Great Barrington Declaration advocated ‘focussed protection’ of the vulnerable, the governments of the world chose unfocussed and imperfect protection.
The latest manifestation of this fundamental strategic mistake is mass vaccination. Governments are still trying to control circulation of the virus through their communities, this time through vaccination. They think that it will not be sufficient to vaccinate the vulnerable, that it will be necessary to ‘vaccinate the world.’ While a large percentage of the population will consent voluntarily, because governments are aiming at universal coverage they resort to coercion of different kinds to reach the marginal 10-20% of the population that is holding out.
Is it feasible to ‘stop the spread’ of a common coronavirus that has spread like wildfire around the world, even through mass vaccination? No evidence has been advanced to support the feasibility of this goal, and the evidence that is available indicates it is unrealistic. Vaccination will not end influenza epidemics and pandemics, nor will it end Covid.
As we draw near to the end of the second year of the pandemic, it is becoming clear that this new universal strategy is again in trouble, just like mass confinement.
Before we consider that however, first let us address the fundamental human rights that are at play here.
The Universal Declaration on Bioethics and Human Rights includes Article 5:
The autonomy of persons to make decisions, while taking responsibility for those decisions and respecting the autonomy of others, is to be respected.
All human rights codes and formulations have loopholes, and Article 27 declares that these rights can be ‘limited,’ ‘for the protection of public health or for the protection of the rights and freedoms of others.’ Even the right to bodily integrity can be infringed on the basis of what Shaman refers to as ‘the prevailing rule that individual liberty could be regulated in any way necessary to promote the general welfare.’
It was on this basis that the eminent philosopher and Professor of Bioethics Peter Singer wrote an opinion piece: ‘Why vaccination should be compulsory.’ He quoted the famous principle from John Stuart Mill’s immortal On Liberty: ‘the only purpose for which power can be rightfully exercised over any member of a civilised community, against his will, is to prevent harm to others.’
First, Singer argues that we are not good at making choices about very small risks and so legal sanctions to prevent this are justified, using the analogy of seatbelt laws. If we don’t make vaccination compulsory, ‘too many people make decisions that they later regret.’ This is an argument for government paternalism. Second, he argues that unvaccinated people do cause harm to others.
Singer is making not one, but three assumptions here: that getting vaccinated with the current Covid-19 vaccines is invariably the right decision for all individuals to protect themselves; that it will not harm them; and that it will also protect others.
The first key point of principle to make is that the right to bodily integrity is so fundamental that it should not be overridden lightly. We might reluctantly concede that there could in principle be a scenario in which there was an outbreak of a disease with a 50% mortality rate or risk of hospitalization, and the spread of the disease could be stamped out by vaccinating all members of the community with a sterilising vaccine that prevented them from infecting others. But this is not the current scenario by any means, as the risks posed by Covid are much lower and differentiated and the vaccines are not protective enough.
The bar for proving that conditions warrant overriding bodily integrity and personal autonomy needs to be raised very high, to prevent unnecessary government overreach. We no longer have the degree of trust in government to get policies right that we had back in the day when seatbelt laws were introduced.
And Singer’s three assumptions need to be checked against the science.
And all codes of medical ethics and human rights are in agreement that informed consent must be given for any medical procedure. Consent must be voluntary, which by definition means it must be obtained without coercion or pressure. For example, the World Medical Association’s Lisbon Declaration on the Rights of the Patient includes: ‘Diagnostic procedures or treatment against the patient’s will can be carried out only in exceptional cases, if specifically permitted by law and conforming to the principles of medical ethics.’ If the patient consents against their will because otherwise they will lose their job, is that permissible, even if a law is passed to make this possible?
Efficacy
First, to what extent do vaccines protect the bearer (so to speak)? Here we are looking for the evidence that they substantially reduce infections, and more importantly severe disease, hospitalization and death.
The first line of evidence is represented by the reports of the clinical trials for the most commonly-used vaccines: the ones from Pfizer, Moderna and AstraZeneca/Oxford University (AZ). They are mainly directed towards establishing that the vaccines are effective at preventing infection, and the headline rates of effectiveness (over 90% for Pfizer and Moderna) address this point although they were magnified by being expressed in terms of relative risk rather than absolute per capita risk. We need to approach the reports of these trials with caution, as they have limited independent input.
The report of the Pfizer trial includes this disclaimer: ‘Pfizer was responsible for the design and conduct of the trial, data collection, data analysis, data interpretation, and the writing of the manuscript.’ Right, so we are dealing with a closed in-house trial and they gave a pre-written report to the expert authors and asked them to sign on the dotted line.
The Moderna report has a similar disclaimer with some more detail, but it still shows a high degree of control by the company over the whole process. We don’t know what the authors were allowed to see as the basis for their assessment of the completeness of the data, let alone how it was analysed.
Peter Doshi, the Associate Editor of the British Medical Journal, raised many issues both before and after publication of these reports, including the treatment of ‘suspected’ Covid cases in the Pfizer trial, the greater need for an analysis of the vaccines’ effectiveness against severe Covid, signs of unblinding in the placebo group and the inclusion of individuals who were already positive at the outset of the trial, who we now know would be highly unlikely to become reinfected. Doshi maintained that resolution of these issues required independent investigators to be given access to the raw data, but none of the companies have done this.
The equivalent declaration for the AZ report shows greater independence from the company so it has more credibility, but the degree of independence from the academic inventors and proponents is not clear.
So, to what extent did regulators subject the applications from the companies for emergency use to independent evaluation? Hardly at all, is the answer. The US Food and Drug Administration’s report for its advisory committee meeting on the Pfizer vaccine asked none of Peter Doshi’s hard questions. Regulatory assessment reports should raise issues, but these reports largely represent the information given to them by the companies and accept it at face value, which is not good enough when so much is at stake. In my ten years of experience writing and overseeing regulatory assessments, I would have sent these back for a complete reworking.
What have we learned about the vaccines since they were released?
As we know, Israel has been the world’s laboratory for mass vaccination using the Pfizer vaccine. Early uncontrolled studies claimed that this had brought about a sharp decline in infections, hospitalizations and deaths, but this decline coincided with the Israeli summer, when you would expect respiratory disease to decline anyway. This is an example of the post hoc fallacy.
With the onset of cooler weather, infections went back up again, climbing precipitously to a new peak 20% higher than the previous one, despite 80% of the adult population being vaccinated. This does not look like success.
A national study of all vaccinated Israelis found that:
the efficacy of the vaccine against documented infection for people aged 60 or older decreases from 73% for those who became fully vaccinated in the second half of March to 57% for those who became fully vaccinated during the second half of January…. A similar decrease in vaccine protection is observed for the other age groups. The efficacy of the vaccine against severe disease for the 60+ age group also decreases; from 91% to 86% between those vaccinated four months to those vaccinated six months before the study.
Given that 50% is the FDA benchmark for efficacy against infection, this is discouraging. Efficacy against severe disease appeared to be holding up better, but was still declining. Other studies have also reported waning efficacy against infection. If Israel is the world’s laboratory for vaccination, then you would have to say the experiment failed.
Singapore is another interesting case study, having largely escaped the levels of infections seen in Europe and the Americas during the first wave. However, infections have gone through the roof in a second wave (more than 300% higher) despite 80% full vaccination and 95% partial vaccination.
A Kaiser Permanente study found that vaccine effectiveness against hospitalization from the Delta variant remained high for six months, while a Public Health England study made similar findings.
A study based on the US COVID-19-Associated Hospitalization Surveillance Network found that during the summer peak of 2021, ‘hospitalization rates were ≥10 times higher in unvaccinated persons compared with vaccinated persons for all age groups.’ Once they came to hospital, however, outcomes were more even:
The number and proportion of fully vaccinated persons admitted to the ICU was similar to unvaccinated persons (60 (20.6%) v. 931 (20.0%), respectively; p-value=0.66), as were results for in-hospital death (7.5%) v. 342 (8.4%), respectively; p-value=0.69).
What about mortality? Most commentators agree there is ‘compelling’ evidence that vaccination greatly reduces severe Covid and mortality. However, they are often referring to the more than 90% reduction in mortality for example in the United Kingdom (UK) from the peak in January to the low point in June 2021. This is another example of the post hoc fallacy, as exactly the same decline occurred in 2020, when no vaccination was available. The seasonal effects on mortality are strong and have recently been validated and explained in this study.
A CDC study found that mortality rates were substantially higher among the unvaccinated, but the differential declined as the Delta variant became more prevalent.
Public Health England presented a valuable report of its EAVE II study based on 99% of the population of Scotland (but pre-Delta dominance), which concluded that for this vaccinated population:
The rate of hospitalisation or death for COVID-19 related illness during the study period was 4·6 events per 1000 person-years (1196 events in total). Over the same period, we calculated the rate of hospitalisation or death from COVID-19 as 8·57 events per 1000 person years (10 282 events in total) in the unvaccinated population in Scotland.
Note however that severe outcomes were much higher in the 80+ age group, reaching a level of 62.8 per thousand person years in the case of the Pfizer vaccine.
Again, the strength of the evidence of efficacy is heavily dependent on the time period chosen for measurement. The combined effect of waning and the growing prevalence of the Delta variant is not always clear. Are we simply delaying and prolonging the epidemic again?
There are several reports that the Israeli hospitals are again overwhelmed, although this news report indicates that the rates of serious illness are much higher in the unvaccinated.
Overall, there is a strong case that vaccination protects against the risk of hospitalization and death for the time being, so the benefits to self seem to stack up.
We now need to balance these benefits against the risk of vaccine injury.
Safety
Safety is a huge topic in itself, and could easily take up a whole article on its own.
The most well-known specific adverse effect is an increase in the risk of myocarditis in young males who have been vaccinated with the mRNA vaccines.
Percentage increases are significant, but the rate of increase can be seen most clearly when represented graphically, most notably in this chart from a study by Diaz et al using data from a US hospital system:
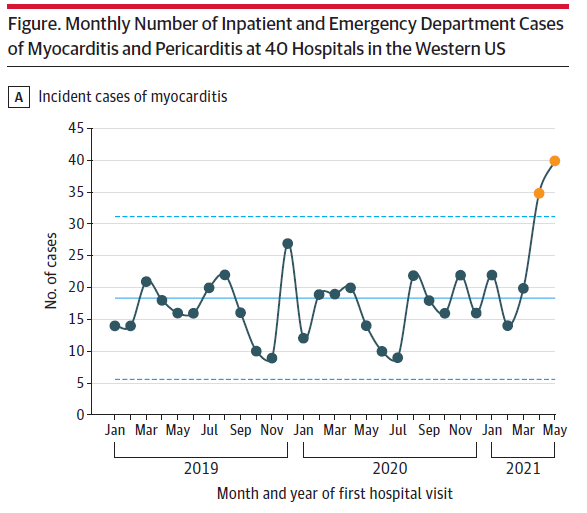
Apologists will argue that myocarditis can be easily treated, but according to King and An: ‘The mortality rate is up to 20% at 1 year and 50% at 5 years.’
There has been much controversy about the mortality figures recorded in the US Vaccine Adverse Event Reporting System (VAERS) which has seen a similar exponential increase in the overall number of total vaccine-related deaths reported in 2020 coinciding with the Covid vaccination campaign.
This has been downplayed on the grounds that the true number of deaths caused by vaccines cannot be determined from this database, which can only be used to find signals. But the increase from the background rates is precisely a signal.
Searching through the data for the twenty years leading up to 2013, Moro et al found a total of 2,149 reports, roughly 100 deaths per year. They concluded that this represents one reported death per million doses. The CDC found that more than 403 million doses of Covid-19 vaccines were administered in the United States from December 14, 2020, through October 6, 2021, during which time, VAERS received 8,638 reports of deaths. This translates to a rate of one reported death per 46,000 doses.
So, the reporting rate for deaths in the year of Covid-19 vaccination is at least 21 times the previous rate. The true differential in reporting rates is probably even greater as the CDC discounted the number of confirmed vaccine-related deaths as compared with the raw data but did this for 2020 only. But the raw data should be used for comparative purposes. Why has there been such an exponential increase?
We can say with total justification that VAERS is generating the biggest signal in history. Is anyone listening? Further investigation is urgently needed, and risk needs to be broken down by age group.
There is clear evidence that the rate of adverse events from Covid is worse than the rate from the vaccines, per capita. For example the Israeli study by Barda et al found that there is an excess risk of 2.7 cases of myocarditis per 100,000 following vaccination, as compared with a higher excess risk of 11.0 cases of myocarditis following infection.
However, this is outweighed by the much higher percentage of Israelis being exposed to the vaccine and in multiple doses. If 10% of Israelis were infected in one year and 80% were given one dose of the vaccine, we would expect nearly 100 additional cases of myocarditis following infection in that country as a whole, and 190 cases following vaccination. Administration of the planned three doses in one year (and possibly later years as well) may lead to higher numbers following vaccination.
We can make similar deductions from a large UK study which found that the incidence of Guillain–Barré syndrome there following infection was 145 per ten million people, much higher than the rate after vaccination with the AstraZeneca vaccine which was only 38 per ten million. But again, out of the total population of 32 million vaccinated people in the study, this would yield over 120 people with Guillain–Barré syndrome following vaccination and only 29 from infection.
The counterargument is that everyone will eventually encounter the virus – however, the whole population will not succumb to infection or illness every year. The way things are heading, a population may encounter the spike protein via vaccines many more times than the wild virus.
So, while rates of adverse events from infection are higher than from vaccination, mass vaccination may lead to higher total numbers of adverse effects in the population of a country as a whole.
The information we have so far about adverse events suggests at a minimum that a more conservative vaccination strategy must be considered, in place of a headlong rush to vaccinate the world. Information about the rates of mortality after vaccination compared with after infection is unknown.
Transmission
Agencies have given up claiming that the Covid vaccines prevent transmission. The evidence shows us there is an initial effect, but it is fleeting and does not last long enough to make any substantive impact on preventing outbreaks or ‘stopping the spread.’
The most specific information comes from a UK study, which found that while there was some initial effect:”’Protection against onward transmission waned within 3 months post second vaccination. For Alpha this still left good levels of protection against transmission, but for Delta this eroded much of the protection against onward transmission, particularly for [the AZ vaccine].”
Riermersma et al found infectious virus in 95% of a subset of samples from 39 vaccinated individuals picked out through PCR testing, a higher rate than for the unvaccinated subset.
A comprehensive Harvard study found: ‘At the country-level, there appears to be no discernable relationship between percentage of population fully vaccinated and new COVID-19 cases in the last 7 days, with similar findings for a large number of US counties.’ Vaccination does not ‘stop the spread,’ as we have seen with the case studies of Israel and Singapore.
If vaccination does not prevent onward transmission, then John Stuart Mill’s test for an infringement of liberty has not been met – the vaccines do not prevent harm to others.
Employers are understandably concerned to ensure that they maintain a safe environment for their employees and remove risks and hazards. But vaccination has not maintained a safe environment overall in Israel or Singapore at the national level. And it cannot maintain a safe environment in workplaces or other venues either because vaccinated individuals can still become infected and pass infection on to others, within weeks, as much as unvaccinated people.
Of course, the safest class of all are the individuals who have recovered from Covid infection. Gazit et al found that the vaccinated were 13 times more likely to become infected compared with those who had been infected previously. Brownstone Institute has collated over 91 studies showing that natural immunity gives at least as much protection as vaccination.
Given that the vaccinated can be infectious, this tells us that the recovered present the lowest risk of all. If there were to be any basis for discriminating in granting people access to workplaces or venues, then first place should go to the recovered, and under no circumstances should they be required to undergo the risks of vaccination when they are already immune.
But discriminating between people based on their medical status should never happen, particularly on the flimsy grounds that have been presented.
Conclusion
Governments have pivoted away from lockdowns towards “lockouts” (in the elegant formulation of the Premier of Victoria, who has designated nearly every worker in the State as authorised workers who are required to be vaccinated).
People at low risk from Covid are being excluded from their workplaces and are losing their jobs, in a way that cannot be justified from a detailed examination of the evidence.
It cannot be justified as a form of paternalism (the State knows best), as the government agencies have not demonstrated an ability to weigh up all the evidence in a detached and impartial manner. We no longer have the same level of trust in government that we had back when seat belts were made compulsory. Seatbelts do not directly harm a certain percentage of people who are required to wear them. The balance between the real risks and benefits to each age group is still uncertain.
Coerced vaccination cannot be justified for the purpose of preventing harm to others, as the ability of the vaccines to prevent transmission is weak and fleeting. This is not a strong enough basis to justify infringing people’s rights to bodily integrity, especially considering the risks of vaccine injury.
Governments are still trying vainly to ‘drive the virus into the ground’ and dominate it, and the virus is still winning. Humanity has eliminated smallpox and was close to winning the battle against polio in 2016 before it bounced back in 2020 (governments will attribute this to the cessation of vaccination programs due to lockdowns, although the majority of cases have in fact been vaccine-derived since 2016).
This tells us two things:
- The polio and smallpox vaccines are much more effective than the Covid vaccines
- If a disease can be eliminated, it can be eliminated through voluntary vaccination campaigns without the need for coercion.
We are in the absurd scenario where the major risk of Covid is faced by the post-working age population, but governments and businesses think the solution is to coerce the working age population into getting vaccinated, even though this demonstrably will not ‘stop the spread’ in the workplace.
The bottom line is that an unknown number of healthy people in the low-risk groups may die as a result of the universal mass vaccination strategy, people who would not have died because of Covid. Governments, employers and advocates need to reflect on this carefully and adopt a more conservative model. If we are going to have a trade-off, it needs to be the most favourable trade-off we can devise.
In a previous contribution, I argued that governments should have taken the path of focussed protection and mitigation instead of suppression in the first phase of the pandemic. They should pursue the same approach going forward and take a more holistic view of mitigating risks, not just the ones in front of their noses.
The Israeli “green passports” are already expiring and the vaccinated are becoming officially unvaccinated again – will they be compelled to renew every six months? And before this pandemic is even finished, the pundits are looking over the horizon for the next one.
The bottom line is we must avoid falling into a permanent biosecurity regime of recurrent discrimination and multiple compulsory vaccinations several times a year, with mounting and compounding risks.
It is time to turn our backs on the fear campaign and return to the time-honoured model in which individuals consider their own risk context and make their own decisions about vaccination in consultation with their medical advisors, without government interference.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








