
In the first year of the pandemic, a team from Otago University in New Zealand (my former university) published an interesting study that provided some explanation for the strong public support for lockdown measures. This support came despite known or predicted collateral harms, including loss of livelihoods, elevated mortality from neglect of other diseases and ailments, “deaths of despair” from greater loneliness, and police abuses.
The answer, they said, is the moralization of restrictions in pursuit of a Covid eradication strategy. People did not take kindly even to mere questioning of the restrictions. With many governments, for example the British, deploying state propaganda to the full to instill fear of the disease and shame all effort to question restrictions, the moralization deepened into sacralization.
This offers a plausible explanation for why people who so warmly embrace the moral framework of diversity, inclusion, and tolerance in social policy settings, ended up supporting vaccine apartheid for those hesitant to get jabbed by shots with worryingly thin efficacy and safety trials before approval for public use.
Jacinda Ardern’s government further reinforced New Zealand’s collective moral fervor by proclaiming its doctrine of the health ministry as the “single source of truth” on anything to do with coronavirus, including public health interventions.
With the passage of time, as evidence mounted of the folly of Zero Covid policy and the accumulating harms it was causing, the New Zealand government was trapped in a prison of its own construction and found it difficult to change course, even after the futility of the entire program became obvious in the data.
Initially, New Zealand attained extraordinarily successful results in keeping Covid under control and was widely lauded – by Anthony Fauci, ABC in Australia, the Guardian, NPR, the New York Times – as a model for hardline policy under decisive leadership (read: in contrast to Bad Orange Man who lived in a white house somewhere in Washington, DC).
In truth this owed much more to several fortuitous advantages attaching to New Zealand. When the first big wave of Covid swept across the world in February–March 2020, it was the height of summer in the Southern Hemisphere. While Covid can infect people in all seasons, it is mostly a winter virus and this gave New Zealand much more of a warning time than was available to Europe and North America.
New Zealand is also a small country of two inhabited islands, which makes border controls much easier to police and enforce, especially with most international passenger traffic coming through one terminal at one airport in Auckland. It is geographically distant from the world’s major international traffic hubs and population centers.
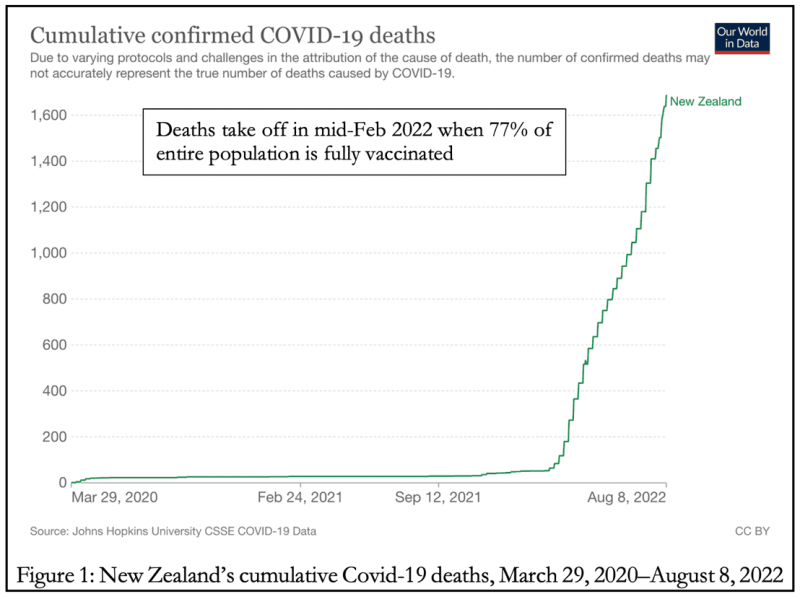
In combination with domestic isolation requirements, the prolonged strict border control measures kept New Zealand’s Covid mortality down to around fifty until the end of 2021 (Figure 1). But by this time Covid was deeply seeded in the world’s major population centers. Accordingly, unless New Zealand were to shut itself off permanently from the rest of the world, an impossible stipulation, the eradication strategy was already doomed.
New Zealand’s strategy had bet the house on stringent measures until vaccines were developed and then the attainment of herd immunity through mass immunization. The bet seemed to have paid off with the development of Covid vaccines in December 2020.
But then the initial efficacy rates of the vaccines, which were granted emergency use authorization long before the standard period for completion of safety as well as efficacy trials, proved to be of exceptionally short duration, necessitating boosters whose efficacy waned even faster.
This meant that the best pathway to herd immunity was through the combination of more robust and longer-lasting natural immunity from prior infection, and vaccines. It also meant that countries that had avoided mass infection through strict isolation measures had built up an immunity debt that left their populations more vulnerable to globally circulating pathogens once they did open up.
And the adverse eventual outcome would only be worsened if, as some epidemiologists had warned, contrary to the professional consensus, a mass vaccination campaign in the middle of a pandemic gave an evolutionary advantage to mutations of the virus with greater vaccine escape properties.
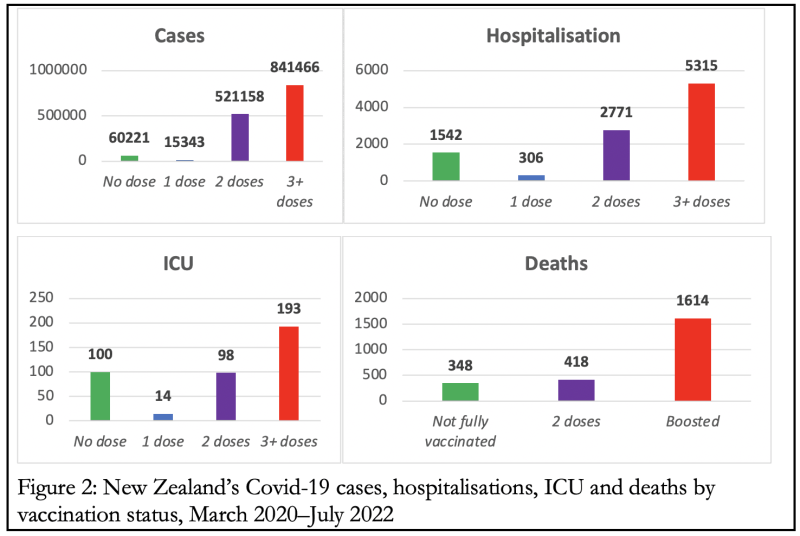
When the far more infectious if less lethal Omicron variant struck New Zealand, therefore, the vaccines developed to combat the original Wuhan strain proved unfit for the purpose of controlling the spread. New Zealand’s cases and deaths really took off in mid-February 2022, despite a vaccination coverage of 77% of the entire population by then (Figure 1). In addition, the greater vulnerability of its population to new viral strains produced some sort of a catching-up effect in the Covid-related case, hospitalization, ICU and death numbers (Figure 2).
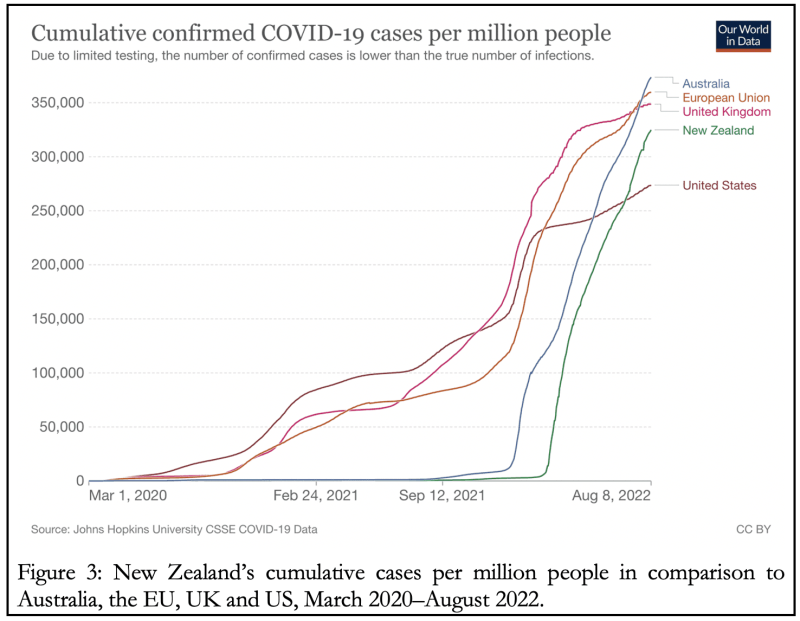
By August 2022, New Zealand’s cumulative Covid-19 cases per million people had surpassed the US and was on track to catch up with the UK and EU. Australia was ahead of all of them. To be fair, though, by this date Australia still had a Covid death toll only about one-fifth to one-sixth, and New Zealand between one-seventh to one-ninth, of the European, British and American figures (Figure 3).
Finally, the little matter of vaccine effectiveness. By August 2022, 80% of Kiwis were fully vaccinated, yet 85.5% of the total death toll was of people vaccinated with 2-4 doses. According to official data from the Ministry of Health (the infamous single source of truth), as at August 9, 2022, the country’s total Covid deaths since February 2020 were 2,413.
People aged over 60 accounted for 91.5% of the total. Covid-19 was officially coded as the underlying cause in 44% of the total deaths, and as a contributory factor in another 24.2%.
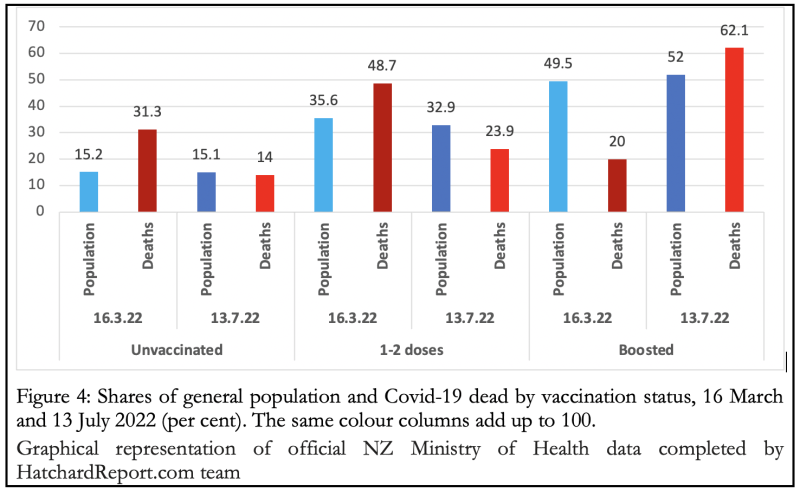
The dramatic turnaround can be seen in Figure 4. As late as mid-March this year, the narrative of a pandemic of the unvaccinated was still plausible, as they comprised more than twice the number of Covid dead compared to their share in the general population, while the boosted dead were only around 40% of their population share.
But in just three months there was a dramatic switch in their proportions. By now the unvaccinated are broadly the same share in the general population and among the Covid dead, while the boosted are overrepresented by almost 20% among the Covid dead compared to their population share. It’s the 1-2 doses cohort that seems to offer the best protection.
According to Jennifer Margulis and Joe Wang writing in The Epoch Times, a couple of recent studies conclude that successive doses of mRNA vaccines can habituate and desensitize the body and in essence, teach it to become more coronavirus spike protein-tolerant. That is, the vaccines convert the body’s natural immune response from protecting the body by attacking the spike protein, to tolerating it as non-threatening.
Yet another explanation of the turnaround since mid-March could be that with mass infections and the resulting naturally-acquired immunity, the vaccinated have lost their ‘competitive advantage’ over the unvaccinated.
Whatever the explanation, as with the case of the state of New South Wales in Australia that was discussed in an earlier article, can we fairly talk of the pandemic of the vaccine-boosted in New Zealand?
For over two years, the Australian Human Rights Commission has been essentially missing in action insofar as the wide-ranging assault on civil rights and political freedoms are concerned. The same seems to have been true of the vast human rights machinery that has grown up in every democratic society that kept prudently quiet rather than confront the unchecked power of the administrative state as it rode roughshod over long-established individual rights vis-à-vis the state.
Recently, however, Australian Human Rights Commissioner Lorraine Finlay wrote in The Australian calling for a reexamination. “The failure to embed human rights considerations into pandemic planning,” she wrote, resulted in “Covid-19 response measures that did not give sufficient weight to human rights concerns.”
Human rights considerations, she concludes, must be incorporated into future emergency planning “as a priority. Even in the middle of an emergency – perhaps especially in the middle of an emergency – human rights matter.”
Yes!
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








