
The World Health Organization, United Nations, UNICEF, non-governmental organizations and governments are all publicly promoting equity, inclusiveness and diversity. At the same time, these organizations were leading lockdowns and mandates that disadvantaged women disproportionately, especially those with a low salary, in health and income.
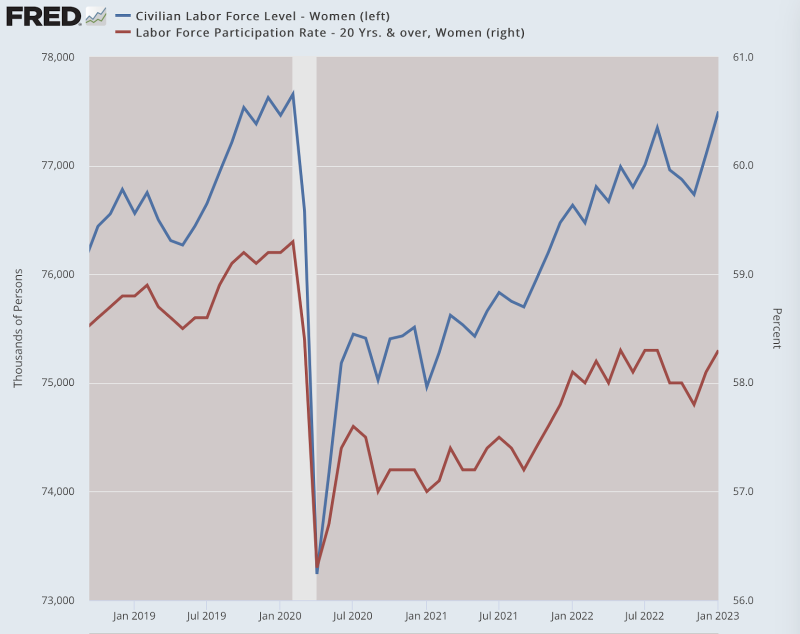
Many of the women who lost paid work have not returned to paid work.
Meanwhile, employed women with disabilities have risen dramatically.
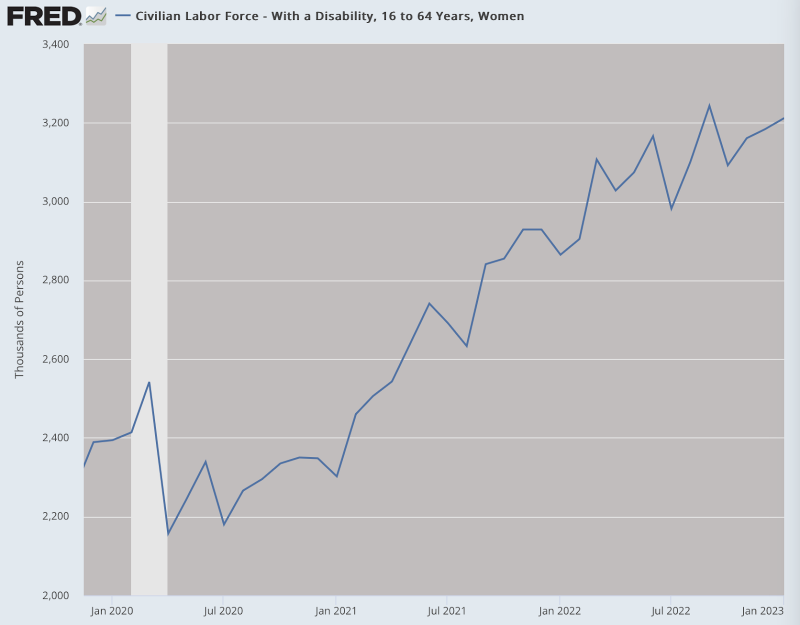
Also among employed Canadians disability rises had the highest prevalence during the pandemic, for women aged (16-54 years). For decades it has been known that women are more likely to have health limitations over their lifetime.
Moreover, the emergence of the Covid-19 pandemic has created an environment where more determinants of poor mental health are exacerbated for women. Disaggregated data on the highest excess mortality and disabilities in women worldwide can be expected.
Psychological stress, fatigue, exhaustion, and high toxin exposures are associated with poor liver function and immunological aging. Immune aging can promote cancer, heart disease and other related inflammatory conditions and reduce the effectiveness of vaccines by an overrepresentation of senescent cells and less naïve cells.
Not a virus but a weakened immune system has become the highest risk for public health caused by various pandemic measures suppressing a healthy human physiology.
Chronic psychological stress
Negative effects of the pandemic measures on mental health will be far-reaching, with women being more affected than men. Women are two times more likely to be diagnosed with depression and anxiety and psychotropic drugs prescribed.
Studies are showing that between 20-70 percent of the health workforce, with women being 70-80 percent of the global paid health workforce) are struggling with mental health issues (stress, insomnia, depression, distress and post-traumatic stress syndrome). Women, especially nurses, have disproportionately been affected during the pandemic.
Unfortunately, health inequality starts in young girls. New research from the Centers of Disease Control and Prevention found that nearly three out five high school girls in the US who were surveyed reported feelings of persistent sadness or hopelessness in 2021, a roughly 60 percent increase over the past decade.
It often seems that medicalization of mental health is occurring among women, without proper investigation of underlying causes.
The latest Women in the Workplace report found that 42 percent of the women said they were always or almost always burned out. That is extremely high and might drive women out of the paid workforce entirely or cause them to dial back their careers to something that is more manageable.
The widespread intensity of burnout has led many women to look for new careers that are less demanding and, in some cases, drop out of the paid labor force entirely. Women experience many hurdles in the workplace, hurdles made worse by the pandemic. Part of the burnout is family-related. Since the pandemic started, women are doing considerably more caregiving of children and elderly relatives than they were before the pandemic.
In many countries women work longer hours a day (paid and unpaid) than men. A Harvard opinion in 2015 “Only the overworked die young” warned of a greater risk for heart attack or stroke in people who are overworked. Women are overrepresented in low wage jobs in sectors that are all large employers for women, women of color and disabled women. These sectors had the first and most long-lasting mandates for mask wearing, frequent testing and vaccinations and are among the most impacted by the lockdowns.
Long Covid
Long Covid symptoms were found to be most increased among healthcare workers and could be related to long-term measures and masking in particular. Women are often twice as much symptomatic and diagnosed than men for Long Covid not only in the acute phase but also at follow-up. FAIR Health Inc, an American health insurance company saw the highest incidence in women aged 36-64 years (40 percent of the total number of Long Covid patients) with memory loss (40.0 percent) and sleep disorders (36.6 percent) being the most common symptoms beyond 2 months of infection.
Drug side effects
Sex differences in the body’s responses to medication have long been overlooked. Until 1995 women were banned for participation in clinical trials, and drugs were mostly tested on males only. Yet, a government report describes eight out of ten of the drugs pulled from the market posed greater health risks for women than men. The issue is compounded because women are frequently disregarded when they express medical concerns.
Women are more likely taking medications (psychotropic medications and birth-control pills) than men and seem to be more sensitive and two times more likely to experience serious side effects. Drug and alcohol use and corresponding side effects are also different for women. Research suggests liver enzymes work at different speeds in men than in women.
Vaccine side effects
An existing body of literature as well as recent studies after genetic Covid-19 vaccine injections and post-bacterial or viral vaccine injection show that females have around a twofold higher incidence and severe Adverse Events (local and systemic reactions) reflecting greater inflammatory responses among females than males.
Generally, adult females mount stronger innate and adaptive immune responses than males. This results in a faster clearance of pathogens and greater vaccine efficacy in females than in males but also contributes to their increased susceptibility to inflammatory and autoimmune diseases. For instance, 80 percent of autoimmune diseases occur in females. Sex differences in immune responses to vaccines could be caused by genetic, hormonal, microbiota, nutritional, and environmental factors, or a combination.
Several studies on the Covid-19 vaccines with people with autoimmune diseases and analysis of an aging population (especially elderly) and frail people reported low protection.
Drug-vaccine interference
The interaction and side effects of the use of multiple medicines and concentrations used is mostly unknown, while some medicine might even have more disastrous side effects than any benefits, as it seems to be the case for psychotropic drugs.
A recent study suggests psychotropic drugs, with immunosuppressant capabilities, interact with the PEGylated LNP of Covid-19 mRNA therapeutics. Medicated severe psychiatric illness showed immune malfunction with limited vaccine response and protection for severe Covid-19 disease.
During the pandemic the use of psychotropic medicine increased most for women. The rapid release of the new therapeutic PEGylated LNP mRNA vaccines heightened the concerns about adverse effects and drug-vaccine interactions. Chemotherapy, anticonvulsants, and anti-malaria were documented to interfere with the mRNA vaccines. Much less was known about other drugs.
A study showed that 42 percent of the vaccinated women experienced menstrual changes. A heavier flow after the shots was more likely to be related to nonwhite and older, hormonal contraception, a diagnosed reproductive condition, fever, or fatigue as side effects or previous pregnancy.
A relation of menstrual length and systemic inflammation have been described in the various phases of fertility. An increase in pre-term stillbirths was observed in the first year of the pandemic. Stroke risk rises in women with recurrent miscarriage, stillbirth and low income, and endometriosis is maybe causally associated with ischemic stroke. Recent studies reported that previous Covid-19 infection significantly increases the risk for adverse events following vaccinations.
Remarkably, the possible negative effects on women’s fertility (menstrual changes) after the Covid-19 vaccine rollout were suppressed by medicine adverse reporting organizations at first reporting. Although a relation with the Covid-19 vaccines or lockdowns has not been proven, an observed decline in newborn babies is worrisome.
The Covid19 mRNA vaccines had never been tested on pregnant women before they received Under Emergency Authorization and were advised by many doctors worldwide for pregnant women. Data from a later Pfizer trial with pregnant women have not been made publicly available
Use of LNP mRNA vaccine should be halted, more investigation is needed
At this stage the risk-benefit of the pandemic measures and pharmacological interventions should be urgently investigated, especially in the context of the seemingly devastating effects on women’s health, in light of an infection that has a current mortality comparable or even lower than that of the flu, and studies showing more deaths from non-Covid like heart infarction or stroke among the once- and two times-vaccinated as compared to the unvaccinated.
Immune exhaustion emerges after a third dose and a risk for autoimmune diseases like Guillaume Barre, Bell’s palsy, Small fiber peripheral neuropathy , a large cluster of myositis, and a potential role of the spike protein in neurodegenerative diseases. In this context, especially the rise in the use of psychotropic medicine, the use of birth pills by many women and their known risk for thrombosis, stroke, heart attack, and sudden death is worrisome. A possible drug vaccine interaction needs to be investigated.
Even public health officials who previously pushed the Covid-19 vaccines recently recognized in a paper published in Cell that deficiencies of the current Covid-19 vaccines became apparent as SARS-CoV-2 strain variants have emerged, questioning whether any vaccine against respiratory viral infections can ever work well enough. The number of medical doctors and scientists speaking out to pause the use of the Covid-19 vaccines for all ages until results of thorough investigations have been made publicly available is increasing daily.
The Covid response caused an economic blowback with long lasting consequences.
Many studies have demonstrated that equal numbers of women and men in organizations and society yield in more well-being, stronger innovation, better decision-making, inspiring workplaces, and economic growth. In the US women’s labor force participation increased threefold since 1920 to 58 percent.
The pandemic policy resulted in the biggest setback in women’s participation in paid work and gender equality for a generation and undermines women’s security and resilience to shocks and ability to pay for health services when needed. An expected further collapsing health system, and at the same time an increase in disabilities and elderly people, suggests that even more women will leave the workforce in the near future to fulfill (unpaid) care and domestic work.
The economic fallout has a harsher impact on women who disproportionately are represented in sectors offering low wages and the least secure jobs.
Globally, women lost $800 billion in income, and accounted for more than 64 million jobs lost in 2021, which is 5 percent of the total jobs of women whereas men had a 3.9 percent loss of jobs. The US IZA from October 2020 suggested that women are 24 percent more likely to permanently lose their jobs than men and their labor income will fall by 50 percent more than men’s. In the health care sector itself, the realms that have yet to recover their losses – nursing homes and long-term care – women entirely dominate in employment.
Health is the biggest economic sector, employing 234 million people worldwide, the majority being women delivering health services to around 5 billion people. The overall employment is expected to grow 13 percent from 2021 to 2030, much faster than other occupations. Its growth is being driven by an increasing number of older people and by the expansion of the global middle class.
Women are 80 percent of the world’s nurses and 90 percent of the frontline health workers. When women’s contribution to all types of care (not just health care) is considered, the immense value of women is rising to $11 trillion or 9 percent of global GDP (Gross Domestic Product). However, women have had enough, as is described in a previous article, the Great Resignation in a Collapsing Health System.
More than nine in ten (93 percent) women have seen a doctor or health care provider in the past two years. One in four (24 percent) women report having had problems paying medical bills in the past months and over half (57 percent) of them say this was due at least in part to the Covid pandemic. Large shares of lower income women report (9-20 percent) being in fair or poor health.
Transformative change for a healthy world
The pandemic proved a society’s reliance on women both on the front line and at home, forming the backbone of society. Women play a crucial role in surviving and preventing natural crises and building strong and resilient communities. In a healthy world it is important women will be heard.
A recovery from the biggest medical disaster in history is an opportunity for change with full participation and the contribution of women in paid work, decision-making and leadership. The priority is investment in safe cost-effective health systems strengthening women’s health and social protection to rebuild trust, public health, and economies with opportunities for all – and no more disruptions such as lockdowns, mask- and vaccine mandates that have so devastated women.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








