
A statistician has come forward with disturbing information that, if correct, will promote doubt on the safety of mRNA vaccination for decades into the future. The whistleblower was involved with building and implementing the New Zealand government database vaccine payment system, a ‘pay per dose system’ that would remit payments to vaccination providers.
In an interview with New Zealand journalist and lawyer Liz Gunn, and using a false name of Winston Smith, the statistician states that science is all about being sceptical and curious at the same time. We shouldn’t be criticised for being sceptical, we shouldn’t be vilified for having a different opinion. We should be allowed to have that.
Smith explained by way of introduction ‘I’m not anti-vax. I helped build the vaccination system. But I am pro-choice and I do believe in [the] fundamental freedoms of humans, and that we should not have a procedure forced onto us because of a mandate just to keep our jobs. That is against everything I stand for. It is a huge overreach by the government.’
Smith’s work also involved data analysis. Smith had noticed discrepancies almost immediately the system went live with people dying within a week of being injected.
Looking at the government data, he ran a query to identify days when more than one hundred and twenty people died in New Zealand. Historic peaks above this level, as Smith demonstrates, are rare. This normal distribution of deaths at this level is only rarely exceeded on the occasional day, or for disaster events, such as the 2011 Christchurch earthquake, mosque shooting in 2019, or an unusually bad influenza season.
In the small country of New Zealand, daily mortality levels that exceed one hundred and twenty could plausibly be considered to be a signal of a disaster event that should trigger public discussion and controversy.
New Zealand had a highly unusual winter flu season in June-July 2019, and no days exceeded the harm-signal level in 2020.
However, in June and July 2021 Smith observed 10 days where mortality exceeded the signal-level. This could be attributed to either COVID-19 or to the injections. Yet not more than a few deaths due to COVID-19 were registered in this time period.
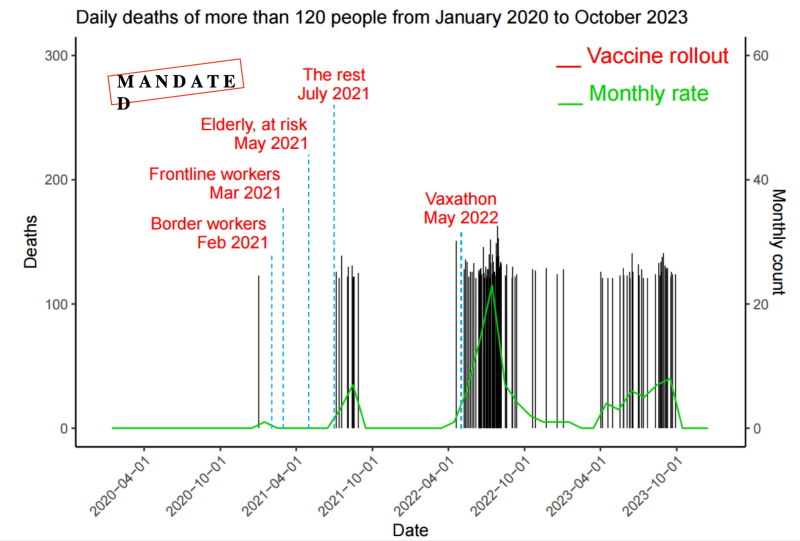
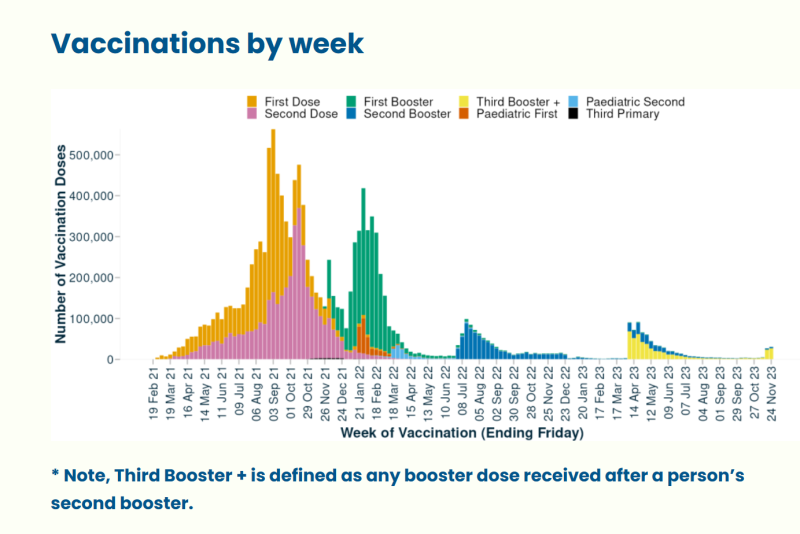
This uptick in deaths coincided with expansion of the vaccine rollout. The mRNA gene therapy was offered to the general public, two million people from July 2021 onwards.
However, by April 2022, as Smith states ‘now the vaccine rollout comes into full effect.’ Booster-injections had peaked in the first quarter of 2022, in the New Zealand summer.
In June 2022 50% of all days exceeded the signal-level with excessive mortality rates rolling into 2023.
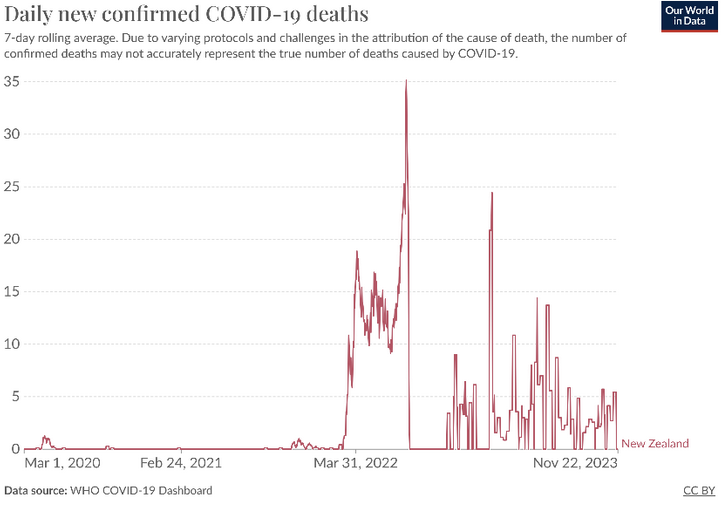
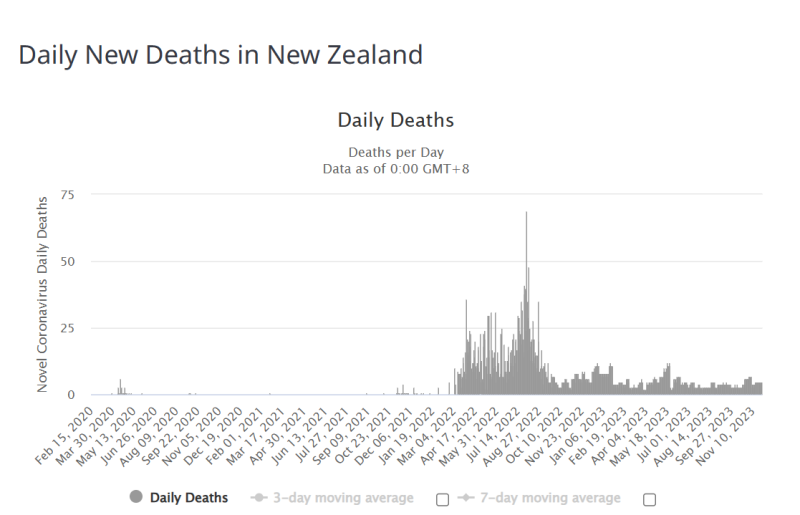
Smith bases his claim that the 2022 data is not muddied by COVID-19 deaths, as SARS-CoV-2 deaths were relatively stable in 2022, rarely exceeding 30 deaths per day and only once exceeding 50 deaths per day, and COVID-19 related deaths dropping steeply off after this date.
Smith claims that there are spikes in unexpected mortality rates in less populated regions outside the capital cities, far in excess of normal background rates.
Of the twenty worst sites, seven of them appear in Christchurch city, a university town with a population of 380,000.

Smith drew attention to one site in Invercargill, a city of 50,000 that he alleges had a vaccine-related death count of 253, following a total vaccine rate on that site, a medical centre, of 837. He claims that ‘one in three people who were vaccinated at this site are now dead.’
I note that in April 2022 media were reporting a spike in Covid-19 infections in Invercargill, but no corresponding death rate. People may have been compelled to get vaccinated in this period knowing the virus was circulating; however, it is plausible that they may have also been exposed to a ‘triple whammy’ of the heart-damaging and inflammatory spike protein following injections, then boosters, and the circulating virus.
Smith’s data suggests that some vaccination sites, including medical centres, pharmacies, and rest homes for the elderly, had extremely high death counts above 20% and at times more than 30% for as many as 800 or 900 vaccinations onsite.
Smith is unclear about the time between injection and death, surmising that it could be up to two months, but adamant that even in the rest homes, the death rate exceeded the normal distribution for the very elderly.
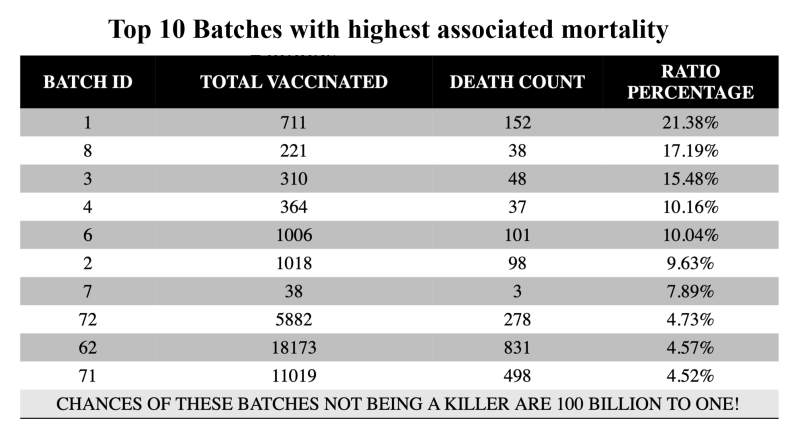
Smith suspects that there could be an issue with batch numbers and irregularities in the vaccine. As a biologic drug, the mRNA gene therapy was always vulnerable to irregularities and contamination.
Smith toggled batch ID numbers with the associated death rate to arrive at a death count and a ratio of deaths by batch. The top ten batches were all Pfizer. (Note: global batch IDs can be sourced from ‘Find My Batch.’)
Registered deaths by vaccinator also suggests that vaccinators (or the batch numbers used by the vaccinators) increased risk, with death by vaccinator up to 25% of people vaccinated.
Deaths would also cluster on particular days, for example in Invercargill, discussed above there were ten clusters of 3-10 deaths per day, and four clusters of 21-30 deaths per day.
Smith maintains ‘this is not natural, this is man-made.’ His IT system has 2.2 million New Zealanders registered, and the natural background mortality rate is 0.75, and all ages are registered. Smith insists that his data suggests not chance, or bad luck, but causality.
There’s so much pain and tears.
Smith had not come forward earlier, because as a scientist, he was aware he required a strong consistent signal in order for his findings to be accepted.
Interviewer Gunn stated, ‘I’d like to remind people. We were sold the jab to protect the old people.’
Smith approached former mainstream journalist and lawyer Liz Gunn to help disclose this information, and the two have worked with a global group of academics and experts to ensure the release of this information was suitably handled.
Smith was in an unusual position as the database administrator for the payment system. ‘Because New Zealand is a small country, you can get away with one database administrator. I am in a unique position, and because New Zealand is a Tier 1 country with really good IT, I was able to manage and build this system.’
Death is the ultimate adverse event… statistically it’s very difficult to disprove this.
If it was settled science we’d be living on a flat earth and we’d be the centre of the universe.’
Smith and Gunn are encouraging experts in data analysis to come forward and look at his data.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








