
The first evidence of lost knowledge in 2020 concerned natural immunity. How in the world did it come to be that people did not generally know that for respiratory viruses, infection and recovery is the best vaccine? This was the counterintuitive wisdom taught for generations in public school in the postwar period. The point was underscored by early exposure to chickenpox. But by the 21st century, it seemed like the knowledge had oddly vanished. Even those with natural immunity were forced to get the shot or lose their jobs.
I wrote at the time that the issue reminded me of the case of scurvy, the cure and prevention of which kept being lost and found throughout history. The standard protocol (lemons) was so effective that people forgot the problem. When the problem reappeared, they forgot the solution.
Apparently this happened with natural immunity too, which is why so many in the population were convinced that hiding under the sofa – reappearing only with a mask to stand in line for a vaccine – was the right solution to a pandemic.
It’s pathetic.
But it’s only the beginning of the chronicle of lost knowledge. Consider the discoveries surrounding the 1918 pandemic. A major research paper from 2008 (with Anthony Fauci as co-author) concluded that:
The majority of deaths during the influenza pandemic of 1918-1919 were not caused by the influenza virus acting alone…. Instead, most victims succumbed to bacterial pneumonia following influenza virus infection. The pneumonia was caused when bacteria that normally inhabit the nose and throat invaded the lungs along a pathway created when the virus destroyed the cells that line the bronchial tubes and lungs.
A future influenza pandemic may unfold in a similar manner, say the NIAID authors, whose paper in the Oct. 1 issue of The Journal of Infectious Diseases is now available online. Therefore, the authors conclude, comprehensive pandemic preparations should include not only efforts to produce new or improved influenza vaccines and antiviral drugs but also provisions to stockpile antibiotics and bacterial vaccines as well.
That research underscored why many of us were persuaded that something like 1918 would never be repeated. After all, we have antibiotics now. The virus can be handled with normal therapeutics and, when that doesn’t work, we handle the second infections with our glorious new miracle drugs (first penicillin and then all the others). Truly, it doesn’t take a medical degree (which I certainly do not have) to understand this.
(To be sure, other research has delved deeper and cited overuse of aspirin as a major factor in 1918 deaths. Once again, we have the miracle cure such as Remdesivir becoming a source of the problem.)
Now we have to fast forward a century later and see more clearly what took place on the medical front in recent history concerning Covid. New research, sure enough, draws attention to the way in which the virus alone was not the most destructive killer. Reports Medical Express:
Secondary bacterial infection of the lung (pneumonia) was extremely common in patients with COVID-19, affecting almost half the patients who required support from mechanical ventilation. By applying machine learning to medical record data, scientists at Northwestern University Feinberg School of Medicine found that secondary bacterial pneumonia that does not resolve was a key driver of death in patients with COVID-19. It may even exceed death rates from the viral infection itself.
In other words: Deja Vu! What happened was a variant of what took place all those years ago. When people said in March 2020 that this new virus reminds them of 1918, they were right in ways that they did not know. It turns out that some of the the same errors were repeated over again, and this was despite all the medical experience and innovations since those days.
The study itself implicates intubation in particular as the driver of bacterial infection. They call it VAP for ventilator-associated pneumonia. But this is not the only source. An untreated outpatient can develop pneumonia or some other associated infection that can end very badly or prolong the period of sickness.
In my own Covid case, I waited far too long to call a doctor. I was fortunate enough to get the great Dr. Pierre Kory on the phone, who did careful diagnostics and prescribed me a variety of medications, among which was an antibiotic. He had by then had a tremendous amount of clinical experience with this virus, and knew all the signs.

Given pharmacies at the time, I was unable to get Ivermectin through regular means, which is a scandal of its own. The NIH/CDC/FDA deprecated early treatment and eschewed any randomized trials for repurpose drugs. This was not an accident. The EUA for the vaccine would only be validated if there were no other options, and therefore other options were taken off the table. This included discouraging pharmacies from distributing drugs they would have otherwise given.
When I did find a source for re-purpose but previously approved drugs, it came in a packet with Ivermectin, Zinc, and Doxycycline, a conventional antibiotic. The package was clearly foreign made. It turns out that these Covid kits were being distributed in most parts of Latin America, India, Europe, and other places.
But they were generally not available in the US. This was a “hide-and-wait-for-the-vaccine” country (and also a “mask-up-when-you-go-out” country), which, as it turns out, is a major reason why the US had such terrible Covid outcomes.
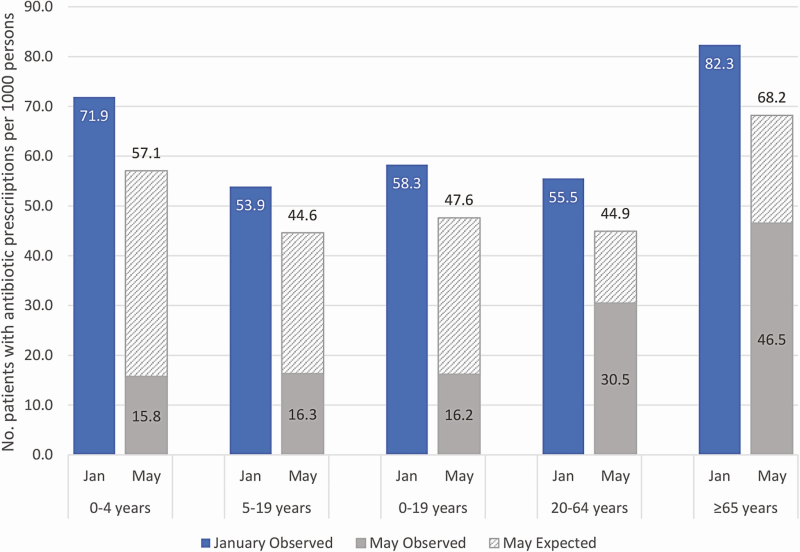
How were these secondary bacterial infections treated in the US? A major study in December 2020 examined antibiotic prescriptions for the worst year of the pandemics. It found:
From January to May 2020, more than 6 million fewer outpatients were dispensed antibiotic prescriptions from retail pharmacies than would be expected based on the same timeframe in prior years. Decreases were seen across all antibiotic classes and agents, with the greatest beyond seasonally expected declines among agents commonly prescribed for respiratory diseases, dentistry, and surgical prophylaxis…. We observed marked beyond seasonally expected declines in outpatient antibiotic prescribing during the COVID-19 pandemic.
To be sure, these could have resulted from less use of the medical system in general due to shutdowns. That alone is weird: that there would be a 30 percent decline in medical spending during a pandemic is a salient fact. And it is probably true that antibiotics are generally overused. That said, one might suppose that if secondary infections were a major cause of death, antibiotic use would at least rise or stay the same. That didn’t happen. Their use declined dramatically.
Putting all of this together, we gain a picture of an incredible scandal. It’s not just that the vaccines did not end the pandemic and proved ineffective against infection and transmission. This should have surprised no one because the Emergency Use Authorization never promised any degree of sterilization from the vaccine.
In addition, there has never been an effective vaccine developed for a fast-mutating coronavirus. Attempting to vaccinate a population for such a thing leads to antibody dependent enhancement among other effects. This was widely known among vaccine specialists at the time. Nothing about the supposedly magic mRNA platform changed that. Indeed, there is evidence that they performed worse than adenovirus-vector vaccines.
But as evidence is rolling in, the jaw-dropping degree of the screwups gets ever more profound. It turns out that the main lesson of 1918 – that you need antivirals and antibiotics to minimize death – somehow did not port their way into public-health knowledge 100 years later, at least not in the US Instead, the choice to intubate patients, causing secondary infections, might not have been treated with the actual medications that were widely available at the time.
All of this adds up to a grim picture of mass but often preventable deaths, all because the system did not work to incorporate the previously existing wisdom we learned from a century earlier. We needed merely to rely on the known information gathered from previous periods of history. The system utterly failed and for reasons having to do with regulatory capture and mass panic. Instead, they embarked on a population-wide experiment that created an unfathomable amount of suffering. And they still haven’t admitted it.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








