I am a young man in my early 20s who became obsessed over the last year with digging heavily into medical literature. The goal? To evaluate the math regarding the covid vaccines’ risks and benefits after myocarditis/pericarditis was confirmed to be associated with the covid vaccines in May/June 2021.
Being in the riskiest age and gender category, I wanted to make an informed decision about whether to take it or not. My employer thankfully did not coerce me and allowed me to calmly consider my personal circumstances, history of prior infection, and the shifting data.
Other young men were not so lucky. They were (and still are) being pressured into taking the vaccines (and even boosters) by the federal government, military, certain state governments, universities, and companies regardless of shifting data and prior covid recovery status. These mandates involve taking a risk to our cardiac health at the expense of loss of education, income, employer-provided health insurance, and other critical social goods.
Seeing my fellow youngsters and other adults be coerced, I decided to investigate whether such measures were justified. The following is the result.
If someone didn’t have covid or the vaccine, there might be a case to consider getting vaccinated. However, I am against the mandates that treat the unvaccinated as second-class untouchables, deny livelihoods, bar them from public accommodations and travel, force them to mask or take tests when others aren’t, or be otherwise blocked from normal participation in society.
People experience a genuine welfare loss when forced to do something against their will. It causes psychological distress, and it sows resentment and distrust. It causes harm. Therefore, the bar for any coercion must be extraordinarily high and an airtight case must be presented for how the coercion both benefits them and reduces harm to others. During the past year, such a justification has not been made.
Below are the common arguments I have seen:
- “The Disease Is Eradicable!” a-la Polio (which we are close to stamping out) or Smallpox which was.
A respiratory virus like covid in animal reservoirs galore is not eradicable and will become endemic – just like the 1918 Spanish flu we’ve been living with since birth.
- “They Achieve Herd Immunity!” – Like that involving Measles where about ~94% of the population must be immune to interrupt the chain of transmission.
There was the hope in the early days that vaccines would provide the immunity needed to block transmission, which is critical for herd immunity.
That didn’t happen.
Israel, one of the first countries to be vaccinated en-masse, experienced one of the world’s highest case rates in August and September 2021. Highly-vaccinated locales like Canada and the UK followed soon. “Herd immunity may well be impossible even if every American gets a shot,” The Atlantic wrote in November 2021 when the mandates were gaining steam. Fauci himself published a March 2022 article in the Journal of Infectious Diseases saying that “classical herd immunity, leading to disease eradication or elimination, almost certainly is an unattainable goal.” This argument thus doesn’t apply.
- People have no right to recklessly endanger others!” – or as one person put it in September 2021 on Quora, “Workers have a right to not be around plague carrying parasites.”
Proponents saying this follow the discredited pronouncements of Dr. Fauci, who explained in the early months of the rollout that for those vaccinated “the risk is extremely low of getting infected, of getting sick, or transmitting it to anybody else, full stop.” This is the main idea behind the adoption of the “test or vaccinate” mandates that Biden’s administration and many companies have adopted for their workforce, some lasting to this day. In reality, these are “leaky” “non-sterilizing vaccines” that do not block transmission, a fact that CDC Director Rochelle Walensky acknowledged in an August 6th 2021 interview with Wolf Blitzer.
Those wanting to be among the vaccinated-only fail to understand that such gatherings can become a covid party and that contracting the circulating coronavirus multiple times over their lifetimes is inevitable. Those concerned have individual options to protect themselves if they wish: vaccines, boosters, N95 masks, monoclonals – and the recent slew of therapeutics.
But nope, the mandate crowd wants to catch it from the vaccinated only.
- “They slow the spread!” – This extension of the previous argument may implicitly acknowledge that while encountering the virus is inevitable, reducing the rate at which people get sick is critical to minimize societal disruption.
I will acknowledge that there was some reduction of transmission with Delta, but will contend that it was nowhere close to what popular pressure may have you believe. But there was a debate to be had then.
Omicron changed everything.
Dr. Cyrille Cohen, head of the immunotherapy lab at Bar-Ilan University and adviser to the Israeli government on vaccine and pandemic response, said with respect to transmission with Omicron, “we don’t see virtually any difference … between people vaccinated and non-vaccinated,” adding “both get infected with the virus, more or less at the same pace.”
Moreover, the Indian Supreme Court recently struck down mandates because “emerging scientific opinion… appears to indicate that the risk of transmission of the virus from unvaccinated individuals is almost on par than that from vaccinated persons” and therefore “cannot be said to be proportionate.” It’s just that contagious.
- “Jacobson v. Massachusetts!” – the 1905 case that upheld states’ authority to compel vaccination.
Citers omit that it was precedent for horrors that followed, especially legalized eugenics through forced sterilization per Buck v. Bell in 1927. Justice Holmes wrote: “The principle that sustains compulsory vaccination is broad enough to cover cutting the Fallopian tubes. Three generations of imbeciles are enough.”
This led to 70,000 forced sterilizations in the United States. And in the Nuremberg trials Karl Brandt, the chief Nazi medical officer and Hitler’s personal physician, cited Buck v. Bell in his defense, as did other defendants. Lovely.
The law involved was for a smallpox vaccine mandate, which was justified for the collective good as smallpox was (1) a scourge with a 30% fatality rate – way higher than covid’s < 1% – and (2) eradicable. The punishment leveled against decliners was nothing compared to what was recently done. Violators were just fined $5 (~$150 in today’s dollars). They were not thrown off their jobs, denied livelihoods, employment, education, nor access to public accommodations like baseball diamonds and museums.
- “They preserve hospital capacity by preventing overruns!” – Thankfully early fears that covid patients would lay dying outside of overflowing ERs never came to pass, even before vaccines and monoclonals were developed.
But suppose there is that concern. Who would fly into hospitals? As the comedian Bill Maher succinctly summarized in a monologue railing for greater precision to be applied to the pandemic:
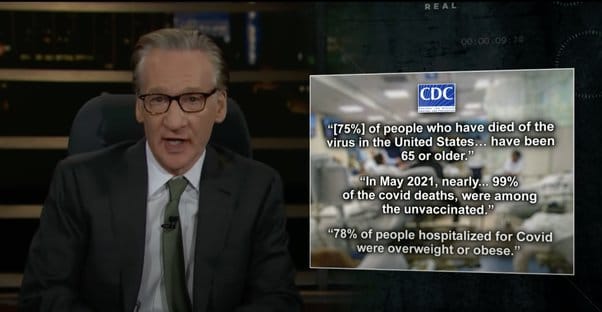
Uptake patterns reflected relative risks. Nearly all vulnerable Americans age 65+ already had at least one dose. The main holdouts were and are younger healthy individuals under 30 with low hospitalization frequency. It may have been a good idea for them to get vaccinated but their reluctance was not exactly self-immolation nor clogging up the ICUs. All coercion is thus misplaced.
- “Previous infection in the unvaccinated does not matter!”
The CDC disagrees. On January 20, 2022 it published an analysis of 22 million positive cases during the Delta wave in California and New York from May 30 to November 20, detailing the rates of hospitalization with severe disease. This is the main metric of concern since these vaccines do not prevent infection – and infection and reinfection cases are inevitable over our lifetimes. It indicates virtually no significant difference between the vaccinated and the unvaccinated with prior infection.
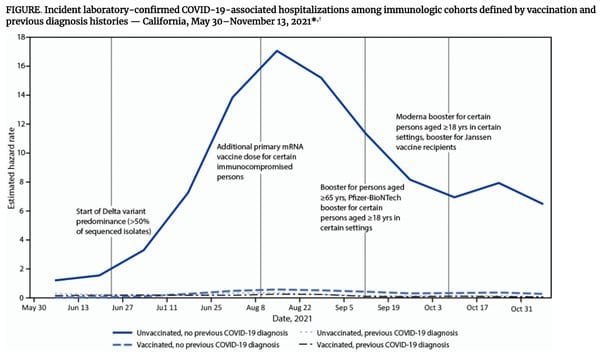
Examining the graph or the paper’s Table I and running the calculations, one will see the risk of hospitalization is lowest in the group that was not vaccinated but previously infected. The following categories are listed with the percentages requiring hospitalization.
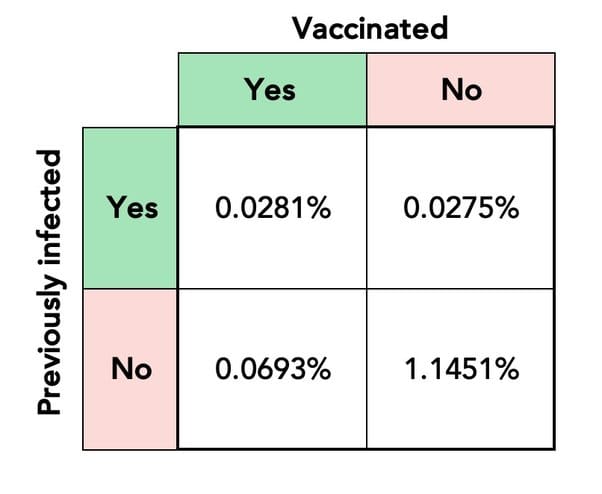
The unvaccinated with prior recovery were more protected than those vaccinated with and without prior infection!
The CDC however dodged open discussion of this result. As Dr. Marty Makary, a John Hopkins epidemiologist, explained in a Wall Street Journal op-ed railing against the costs of public health policy’s refusal to acknowledge prior infection, the CDC spun the narrative to assert “that hybrid immunity – the combination of prior infection and vaccination – was associated with a slightly lower risk of testing positive” but “those with hybrid immunity had a similar low rate of hospitalization (3 per 10,000) to those with natural immunity alone.” Hospitalization risks remained unchanged.
Makary is not the lone voice confirming the power of prior infection.
The distinguished vaccine expert Dr. Paul Offit recently co-wrote an op-ed with former FDA employees Luciana Borio and Philip Krause concluding that it would be wise “for public health authorities, including the CDC, to acknowledge that a coronavirus infection is at least as protective as two doses of vaccine” and that institutions mandating boosters can only require one additional shot.
Others questioning the need to vaccinate the previously-recovered are Drs. Martin Kulldorff (Harvard epidemiologist and biostatistician), Vinay Prasad (hematologist-oncologist and associate professor of epidemiology and biostatistics at the UCSF), Harvey Risch (Yale epidemiologist), and Jayanta Bhattacharya (Stanford epidemiologist). Dr. Monica Gandhi (professor of clinical medicine at the UCSF) holds that firing the unvaccinated with proven prior infection is a step too far but believes one additional dose is the right approach, particularly in those 60+. Eric Topol (head of Scripps Research) acknowledged that the refusal “to acknowledge the evidence has unnecessarily fueled divisiveness and a war against mandates” and advocates for a blanket one dose policy.
So Why Have the Recovered Not Been Treated Differently?
I will return to our friend Paul Offit, who sits on the FDA advisory committee and makes vaccines himself. Most are familiar with his zealous advocacy for vaccinations and mandates both before and during the pandemic. Fewer know that he conceded from the get-go that it was reasonable for the recovered to not want to be vaccinated. When asked on the viral ZDoggMD interview show what he would say to someone who asks: “Why should I be forced, compelled, mandated to get a vaccine when I have gotten natural COVID?”
Offit answered, “I think that’s fair. I think if you’ve been naturally infected, it’s reasonable that you could say, ‘Look, I believe I am protected based on studies that show I have high frequencies of memory plasmablasts in my bone marrow. I’m good,’ I think that’s a reasonable argument.” The problem, as Offit noted in another interview, “is that bureaucratically it’s a nightmare.”
But bureaucratic problems are not Science™on whose behalf public health professes to speak. And as compared to what? Immune people fired and permanently resentful of public health? When asked whether there might be a test that can prove COVID recovery, Offit explained that there is a blood test for antibodies to the virus’ nuclear protein, which could show up if someone has had the virus and is now immune. Imagine how much mental anguish, societal disruption, and divisiveness would have been avoided if among the trillions spent – of which billions were stolen – some was spent on making these tests widely available.
The problems don’t end there. In a January 25, 2022 interview, Offit related how he and three other outside advisors were called into a secret meeting with Drs. Walensky, Fauci, Collins, and Murthy and other top public health officials to consider whether natural infection should be considered in the context of vaccine mandates. A straw poll was held that narrowly decided against such, in a decision that was “bureaucratic more than anything else.”
This sealed the fate of millions of naturally immune, with them either suffering discrimination, mental distress as employers coerced them into an unnecessary medical procedure, and even losing their jobs.
Suppose for the sake of argument that you accept natural immunity as equally good or better than vaccine-induced immunity in protecting from severe disease. What are the ethical consequences? Vaccinating the recovered without informing them that they don’t need it violates both the principles of informed consent and the classic medical ethic of not treating without necessity. Doses are wasted on the immune instead of saving the lives of the vulnerable in developing countries.
Those coerced are subject to the risks of an unnecessary medical procedure, including serious cases of heart inflammation that young men ages 16-24 are particularly susceptible to at a 1 in 3,000 to 6,000 rate. There is also increased psychological reactance and distrust of public health and the medical system among the coerced and broader public who know this coercion to be unscientific and unfair.
Is this what public health should be?
Now one can see why I have nothing positive to say regarding these mandates nor their supporters. The same people who threw around the slogan “Your liberty ends where my nose begins” – many of whom are now up in arms regarding abortion and bodily autonomy – failed to build a bulletproof case for violating others’ autonomy, ran around and bloodied their noses by threatening to throw them off their jobs and make them and their children starve. In multiple instances, the threats were actualized.
And this coercion troubles even some of those most invested in the success of vaccines.
“If you force something on people, if you coerce somebody to do something, that can backfire. Public health has to be based on trust…. these vaccine mandates, and vaccine passports, this coercive thing is turning a lot of people away from vaccines, and not trusting them for very understandable reasons,” says Martin Kulldorff – one of the world’s leading epidemiologists, a specialist in vaccine safety, and consultant to the ACIP COVID-19 Vaccine Safety Technical Subgroup.
“Those who are pushing these vaccine mandates and vaccine passports — vaccine fanatics I would call them — to me they have done much more damage during this one year than the anti-vaxxers have done in two decades. I would even say that these vaccine fanatics, they are the biggest anti-vaxxers…. They’re doing so much more damage to vaccine confidence than anybody else.”
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.