
The Advisory Committee on Immunization Practices (ACIP) of the United States Centers for Disease Control and Prevention (CDC) met recently to discuss, among other topics, the appropriateness of giving Hepatitis B vaccines to all babies in the United States on their first day of life. This practice has been in place for decades, and is in some ways a bit like frontal lobotomies – people just trusted that it was a good idea as otherwise, doctors would not have recommended it. And who wants to argue with health staff on the first day of their baby’s life?
The committee recommended that parents delay Hepatitis B vaccination for at least 2 months, a decision that provoked a fascinating reaction from many prominent doctors who see this as putting babies at risk, or at least their own bruised egos and reputation. If the average American does pay enough attention to read and think through this issue, they will probably be confused. They would be right to be. We all should be.
Much of the hype and argument has been around safety and effectiveness of the vaccine. People will never agree on this, as there is too much at stake for the vaccine industry (lots of money) and too many people annoyed about the money made from vaccines during Covid-19.
Resultant extreme and irreconcilable positions range from all vaccines being intrinsically safe and effective in virtually all people (biological magic) to viruses (and Covid) not even existing in the first place. A congenial debate over a beer won’t bring reconciliation, as neither side has interest in being congenial. Both claim the other is set on killing humanity.
However, these claims are mostly irrelevant to the Hepatitis B vaccines debate. It is really about logic. As the average person, given a couple of minutes, will figure out.
Hepatitis B is transmitted by direct contact with the blood or body fluids of other people who have a current Hepatitis B virus infection. It causes liver inflammation and can lead to chronic liver scarring (cirrhosis), liver failure, and liver cancer, all of which can kill you.
There are no good treatments to get rid of the virus. It can also remain virtually symptomless and harmless in other people, such that they never know they are infected (but we have good tests).
In some countries it is relatively common, such as some Pacific Island nations and some Asian states. However, it is very uncommon in the general population of the United States, being mostly confined to people who inject drugs or have unprotected sex with multiple partners. It is also transmitted within families, at time of birth from the mother, or (for example) if one infected person is bleeding and a family member attends to their wound while having a skin sore of their own.
So, if your parents and siblings are Hepatitis B negative (it is easy to do a blood test to check), then in the US you are really, really unlikely to become infected until you start shooting up drugs or having lots of sex, or maybe working as a trauma surgeon or a paramedic.
Not many US citizens do any of these things in their first two months, or decade, or so. Pregnant women are also routinely tested for hepatitis B (and fathers can be) so we know, when a baby is born, whether there is any risk from family members.
The other relevant thing to understand is that an infant on its first day of life does not have a mature immune system and relies heavily on antibodies obtained from its mother before birth (and some from breast milk). This is partly why we wait a couple of months or more before giving vaccinations against other infections. You would only want to give at birth, amidst all the stresses and rapid changes the baby is undergoing, if immediate risk of an infection was high, such as if the mother had tested positive.
So, most Americans will never be exposed to the virus in their lifetimes, which is why the vaccine was originally restricted, rationally, to people at high risk such as those injecting themselves with illicit drugs, some sex workers or people with many sexual partners, the medical and nursing professions who cut such people up and stitch them back together, and the few babies born to infected mothers (in which case it is quite effective).
There are a lot of unknowns regarding Hep B vaccination on day one of life, as there were never any serious trials on this unique age-group. Just a few hundred babies followed for up to less than a week in the regulatory trials for the two vaccines on the US market.
Other trials were conducted in older age groups, but babies just transferring from placenta to the out-of-womb world are not the same and important things like the permeability of the blood-brain barrier will be different – exposing their developing brain to the various adjuvants and preservatives, including aluminum salts that we know are somewhat neurotoxic. This is why we were always, before Covid addled medical brains, very careful about giving drugs to pregnant women and newborns.
So why did we in the US give Hepatitis B vaccine on day one of life when most countries similar countries don’t? It is not logic, evidence-based medicine or some grown-up rational public health policy. The most likely reason, as most people can readily deduce, is money.
Pharmaceutical companies exist for reasons other than altruism, just like banks and washing machine manufacturers. They are there to make a profit – for their owners who are usually large investment houses and very rich individuals (shareholders), and for their executives. This is, unequivocally, why CEOs and senior staff are appointed by company boards. If these executives don’t perform but just go around worrying about the greater good, they are replaced. It is our model for commerce.
For the same reason (profit), pharmaceutical companies invest in medical schools and encourage curriculums that imply, quite falsely, that vaccines are the main reason people in rich countries live longer today (it’s unequivocally mainly nutrition, sanitation, living conditions and antibiotics, and vaccines that came after most infectious disease death had gone away). They sponsor professional medical societies, who then play the same game.
If you start a measles mortality graph from the year mass vaccination started, there is a strong positive association with reduced measles deaths. This is now popular in journals and medical schools. The same association can be seen between measles deaths and the consumption of cornflakes.
In both cases, it is because measles deaths started dropping rapidly long before and kept on the same trajectory (likely mainly due to better nutrition). Measles vaccination is still great at stopping infection and transmission and therefore some residual measles deaths (so are vitamin supplements in breakfast cereals). Vaccines just came late in the game. In poor countries with malnourished kids, measles vaccines may have more impact. This is a good example of the fallacy that vaccines transformed life expectancy in the United States, and postponing them will kill lots of kids. It won’t.
The companies, holding return on investment as their priority, also design and sponsor their own drug trials, and offer senior staff of regulatory agencies like the FDA (whose salaries they already fund through fees paid by Pharma) the prospects of better-paying jobs if they all remain friends. They can sponsor disease modeling to show far higher mortality than real life can provide, and medical journals to publish fairy tales in support of this cause. They sponsor most members of the US Congress for the same reason. None of this is complicated – it is business and nearly everyone understands it.
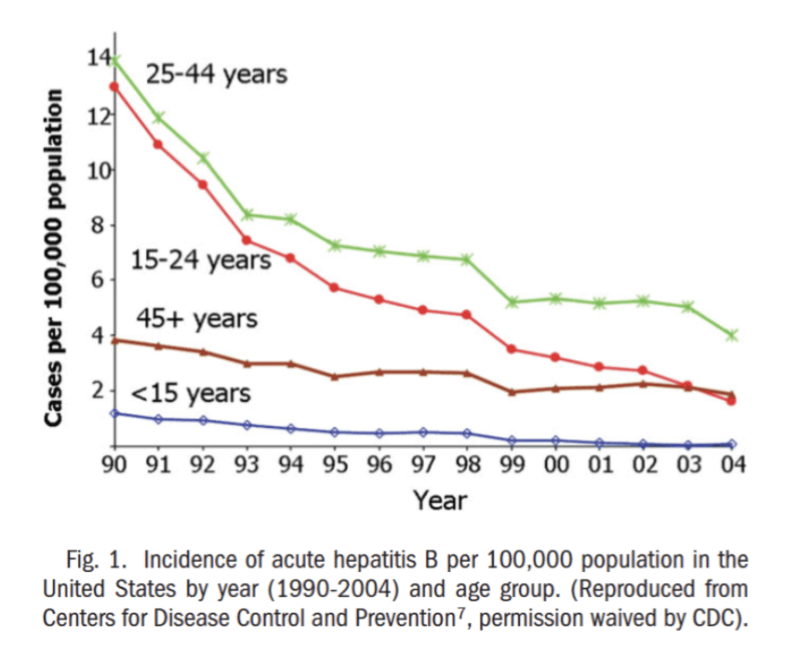
It’s the same with Hepatitis B vaccination. People annoyed at ACIP pointed out that hepatitis B dropped in the US from the time mass infant vaccination was introduced in 1991. However, this was mainly in age groups much older than those affected by infant vaccination, and was almost certainly already happening, as shown in the graphic below.
Why? Increased reluctance to share needles, needle exchange programs, safer sexual practices, more gloves worn for minor medical procedures, and probably also well targeted vaccination at those high-risk groups. The people who said the decline was primarily due to infant vaccination could not have been experts, because they do not apparently understand these concepts and data that the average American will immediately comprehend.
So, ACIP has suggested that newborns with essentially zero risk of contracting Hepatitis B don’t get the hepatitis B vaccine. Commonsense, hard to argue with. However, they do suggest to consider it at 2 months, which still seems illogical from a risk viewpoint (as noted, few babies of that age are shooting up in the back lane or working as trauma surgeons). However, this is roughly the age that many European countries also start, so at least it feels less inept.
Vaccines are medicines – the benefits outweigh the risks for some people (e.g. babies of hepatitis B positive mothers), and the risk outweighs the benefits for a few others. When the disease being avoided is quite rare, that ‘few’ who are harmed actually becomes really important (basic, basic statistics and probabilities that almost everyone understands).
The onus therefore is now on those proposing the medicine to demonstrate the overall benefit. ACIP recognized that we don’t have that for mass newborn vaccination of hepatitis-B-negative parents in a general US context. We don’t at 2 months either.
ACIP was still erring on the side of Pharma, which they presumably have to due to the sponsored-Congress problem. They may have got it right, they may not have. Now the onus is on someone, preferably an independent body like the CDC is supposed to be, to do sensible, well-designed, well-managed, transparent prospective trials in the right populations. It is possible. Only a risk to corporate income and return on shareholder investment could render that idea controversial.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








