
The publication by Gurdasani and others [Gur+22] (British Medical Journal, August 2022) brings much needed focus on the well-being of children, by means of an analysis of the UK’s Covid-19 response related to children and schools. There is however one main aspect on which the paper needs correction.
Intervention needs evidence: In any policy response, it is an active intervention which needs evidence, while “no intervention” (i.e. normality) should be the default. A stronger form of this is that interventions which cause harmful disruption need even stronger scientific evidence. The writeup [Gur+22] flips this principle on its head, by asking for evidence for normality, while providing no or only weak evidence for harmful and disruptive intervention.
Importantly, it must be noted that disruptions have harmed children far more than the SARS-CoV-2 virus. The very first sentence of the writeup claims that children have been severely affected by Covid-19, whereas the entire remaining paragraph lists not harms caused by the virus, but by disruptive policies. Indeed, not only in the UK, but in most of the world, disruptive Covid-19 policies have affected children far more than the virus itself.
Below, we point out various policy aspects and interventions advocated by the writeup [Gur+22], where only weak or incorrect evidence has been offered.
Weak, incorrect evidence on SARS-CoV-2 harming children
The foremost reason for possibly disrupting children’s lives should be for their benefit. Therefore the question of whether the SARS-CoV-2 virus has affected children is paramount. The only real evidence offered by [Gur+22] toward this is in Table-2 of [Gur+22] where 92 deaths with Covid-19 on the death certificate is mentioned.
However, note that Covid-19 largely affects those with serious comorbidities (among children or adults). Also, in many instances, adults or children test PCR positive after being admitted for some other ailment [DY21]. Therefore, the right question is: has Covid-19 caused excess deaths compared to what would have been caused without SARS-Cov-2, i.e. in prior years?
Table 1 lists the total number of deaths in EuroMoMo countries [Eur22] in the age-groups 0-14, 15-44, 45-64, and 65-plus age-groups, in the four years 2018-2021. Now, the total deaths is the most important metric of a pandemic. By this metric, it is clear from the table that those under-45 have not had a pandemic. So overall, the evidence offered by [Gur+22] for SARS-CoV-2 having harmed children is rather weak, and insufficient to justify disruptions to the lives of millions of children.
| Total deaths in 2018 | Total deaths in 2019 | Total deaths in 2020 | Total deaths in 2021 | |
| 0-14y | 19,601 | 19,527 | 17,858 | 18,568 |
| 15-44y | 82,152 | 80,043 | 82,120 | 83,808 |
| 45-64y | 457,204 | 446,954 | 468,148 | 483,815 |
| 65+y | 3,134,658 | 3,118,136 | 3,430,468 | 3,402,766 |
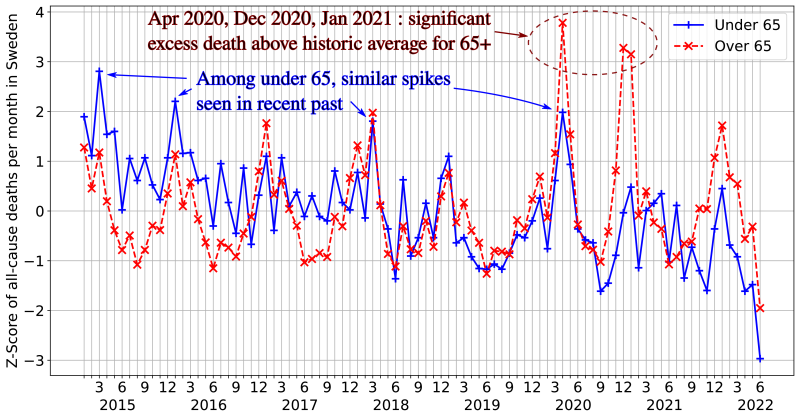
A look at data from Sweden, where children’s lives were least disrupted, and primary schools open throughout, is revealing. Figure 1 shows the z-score of the monthly deaths in Sweden, plotted separately for the under-65 and for the over-65 age-groups (data source: [Swe22]).
Note that the absolute number of deaths in the over-65 population is about 5/6 of the total deaths; the z-score is agnostic to the absolute value as it is a normalized metric. The figure clearly shows the Covid-19-related spike in the months of April 2020, December 2020, and January 2021. But this is in the 65+ age-group. In the under-65 age-group, there is a spike seen in April 2020, but its magnitude is similar to that of spikes in the same age-group in recent prior years. Specifically, the spikes in March 2015 and January 2016 are larger than, and the one in March 2018 comparable to, the spike in April 2020.
On long covid: The other metric presented in Table-2 of [Gur+22] toward the claim that Covid-19 has affected children is the number of long-covid instances. However, given that long-covid symptoms are related to depression, they could as well be caused due to the disruptions to normal life rather than by the virus itself [Mat+22].
No evidence on SARS-CoV-2 elimination
The writeup [Gur+22] claims that “mitigations only delayed rather than prevented impact was flawed,” but cites no evidence to support this. SARS-CoV-2 can infect humans without showing symptoms or only mild symptoms. It also has other species as hosts [Bar21; Jac21]. Therefore its elimination is rather wishful and highly impractical. On the same count, the very first question raised in the writeup [Gur+22] for public inquiry, on preventing Covid-19 in children is a moot one.
Weak, incorrect evidence on children, schools being Covid-19 spreaders
The writeup [Gur+22] repeatedly asserts that children and schools are important spreaders of SARS-CoV-2, but the evidence offered here is weak, even erroneous.
- While some references (15, 16, 18 in [Gur+22]) are based on model-fitting with numerous confounding factors, others find contradictory results: over half the studies considered in reference 24 of [Gur+22] either find that schools are not important spreaders, or do not consider schools at all.
- Reference 25 in [Gur+22] is cited as though children are important SARS-CoV-2 spreaders, whereas the study, which was based in the UK, in fact concludes that there was no “materially increased risk of covid-19 mortality” for adults living with children [For+21].
- Reference 20 is cited by [Gur+22] to support that schools are important SARS-CoV-2 spreaders, is a study from Sweden; this ignores the fact that there has been negligible or no excess mortality among under-65 in Sweden (see Figure 1) or among under-45 in the EuroMoMo countries (see Table 1).
Therefore the references cited by [Gur+22] toward children or schools being SARS-CoV-2 spreaders can hardly be called strong evidence justifying harmful disruption of children’s lives in terms of school closure or isolation protocols.
Weak, incorrect evidence on testing and isolation
On need and effectiveness: The writeup argues that masking and testing should have been required for primary school children (row for “February 2021” in Table-1 of [Gur+22]). It claims that “those living in households with primary school age children were at higher risk of infection,” and references 34-35-36 are cited as support. However, neither reference 34 nor reference 36 present any data to support the above claim. And indeed, reference 35 in fact negates the above claim, by concluding “there is no significant evidence to suggest that schools are playing a substantial role in driving spread in the community.”
On lack of harm: In Table-2 of the writeup [Gur+22], the authors claim “overall mental health did not change.” This simply does not match up to the reality of mental health crisis among children and youth in the UK [Wal21] as well as the USA [Shi21].
Weak, incorrect evidence on masks
On need and effectiveness: The writeup [Gur+22] cites four references (number 62, 70, 71, 78) as support for the claim “masks were effective in reducing transmission, including in school.” However, none of these is a randomized controlled trial. References 70, 71, 78 are population-wide statistics with several confounding factors. And indeed, reference 62 refutes the claim by concluding “No instances of child-to-adult transmission of SARS-CoV-2 were reported within schools.” Once again, while strong evidence is needed for the active intervention of masking, the provided evidence is weak and even contradictory.
On lack of harm: The writeup [Gur+22] cites two publications, references 77 and 79, to support the claim that children are not harmed by the wearing of masks. Both these are studies which measure children’s ability to recognize emotions in one-off settings. This is hardly sufficient evidence to support lack of harm in overall learning, peer-interaction, and social development, when facial expressions are hidden for the majority of school duration.
Weak evidence on Covid-19 vaccines for children
While any intervention needs strong evidence of benefit versus harm, this is even more so for irreversible medical interventions, such as vaccination. Such strong evidence is lacking for Covid-19 vaccination for children. It is telling that the writeup [Gur+22], while arguing for Covid-19 vaccination of children, has not cited a single study to show that benefits outweigh the harms. Indeed, given the extremely low risk of severe Covid-19 outcomes in children, the trials cannot possibly show such a risk-benefit balance [PPB21].
The writeup [Gur+22] argues for children’s Covid-19 vaccination based on measurements of antibody titre. But this is weak evidence, and other prior vaccines based on antibody levels have backfired in terms of disease outcomes, e.g. RSV [CHI+69], Dengvaxia for dengue [Pul21].
Summary
In summary, the lack of strong evidence for any of the interventions and harmful disruptions to children’s lives implies that such interventions were not justified. As the authors of [Gur+22] point out, it is indeed true that children have been weaponized. However, this has been done not by those advocating a normal, enjoyable, and disruption-free childhood for today’s children, but by those advocating for more restrictions on children for the benefit of adults, restrictions for which evidence is weak if any.
References
Adam Barnes. 13 gorillas in US zoo test positive for COVID-19. Sept. 13, 2021. url: https://thehill.com/changing-america/well-being/prevention-cures/571939-thirteen-gorillas-in-us-zoo-test-positive-for/ (visited on 08/13/2022).[CHI+69]
JAMES CHIN et al. “Field evaluation of a respiratory syncytial virus vaccine and a trivalent parainfluenza virus vaccine in a pediatric population.” In: American Journal of Epidemiology 89.4 (1969), pages 449–463.[DY21]
Laura Donnelly and Harry Yorke. Exclusive: Over half of Covid hospitalisations tested positive after admission. July 26, 2021. url: https://www.telegraph.co.uk/news/2021/07/26/exclusive-half-covid-hospitalisations-tested-positive-admission/ (visited on 08/25/2022).[Eur22]
EuroMoMo. EuroMoMo: Graphs and Maps. May 2022. url: https://www.euromomo.eu/graphs-and-maps.[For+21]
Harriet Forbes et al. “Association between living with children and outcomes from covid-19: OpenSAFELY cohort study of 12 million adults in England.” In: BMJ 372 (2021). doi: 10.1136/bmj.n628. reprint: https://www.bmj.com/content/372/bmj.n628.full.pdf. url: https://www.bmj.com/content/372/bmj.n628.[Gur+22]
Deepti Gurdasani et al. “Covid-19 in the UK: policy on children and schools.” In: BMJ 378 (2022). doi: 10.1136/bmj-2022-071234. eprint: https://www.bmj.com/content/378/bmj-2022-071234.full.pdf. url: https://www.bmj.com/content/378/bmj-2022-071234.[Jac21]
Andrew Jacobs. White-Tailed Deer in Iowa Widely Infected With Covid, Study Found. Nov. 2, 2021. url: https://www.nytimes.com/2021/11/02/science/deer-covid-infection.html(visited on 08/13/2022).[Mat+22]
Joane Matta et al. “Association of Self-reported COVID-19 Infection and SARS-CoV-2 Serology Test Results With Persistent Physical Symptoms Among French Adults During the COVID-19 Pandemic.” In: JAMA Internal Medicine 182.1 (Jan. 2022), pages 19–25. issn: 2168-6106. doi: 10.1001/jamainternmed.2021.6454. eprint: https://jamanetwork.com/journals/jamainternalmedicine/articlepdf/2785832/jamainternal\_matta\_2021\_oi\_210066\_1647627389.165.pdf. url: https://doi.org/10.1001/jamainternmed.2021.6454.[PPB21]
Wesley Pegden, Vinay Prasad, and Stefan Baral. Covid vaccines for children should not get emergency use authorization. May 7, 2021. url: https://blogs.bmj.com/bmj/2021/05/07/covid-vaccines-for-children-should-not-get-emergency-use-authorization/ (visited on 09/12/2022).[Pul21]
Jacob M Puliyel. Like Icarus, are we flying too close to the sun with a DNA vaccine against COVID-19? Sept. 20, 2021. url: https://caravanmagazine.in/health/the-little-discussed-risks-of-dna-vaccines-against-covid19 (visited on 09/12/2022).[Shi21]
Deepa Shivaram. Pediatricians say the mental health crisis among kids has become a national emergency. Oct. 2021. url: https://www.npr.org/2021/10/20/1047624943/pediatricians-call-mental-health-crisis-among-kids-a-national-emergency.[Swe22]
Official Statistics of Sweden. Population Statistics. June 27, 2022. url: https://www.scb.se/en/finding-statistics/statistics-by-subject-area/population/population-composition/population-statistics/ (visited on 07/03/2022).[Wal21]
Katie Walderman. Children’s mental health: ’The type of self-harm is the worst we have seen.’ Dec. 2021. url: https://www.bbc.com/news/uk-england-merseyside-59576669.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








