The New Zealand legacy media have spent the past month emphasising the need for ‘face coverings’ or masks in community settings, particularly in schools. They’re carrying this activity out via narrowly framed articles, which don’t accurately reflect public health norms, and certainly don’t reflect conceptions of risk outlined in the scientific and scholarly literature.
What we observe here is New Zealand’s legacy media effectively manufacturing ignorance in service of mask mandate crackdowns that serve the purposes of already-published secondary legislation. This is occurring through a small coterie of message makers and Ministerial power-brokers, rather than through broader, democratic processes.
With regards to mask crackdowns, the message makers appear consistently unable or reluctant to make a critical public health distinction– most mask data demonstrates that prevention of disease is based on vulnerable and unwell populations wearing masks to protect themselves. If there is no meaningful difference on rates of hospitalisation and death, imposing mask mandates on not-at-risk populations is arbitrary and cruel.
That our media would simply repeat the ‘infection’ narrative, at this stage, when data has long demonstrated that the majority of the population are not at harm from infection, is a public health debacle.
Evidence that community-level mandated masking meaningfully prevents hospitalisation and disease is weak. Healthy populations should not be coerced, through social, political, and regulatory pressure, to comply with a medical intervention that makes no meaningful difference, while ignoring interventions that may make greater difference for those most at risk of harm.
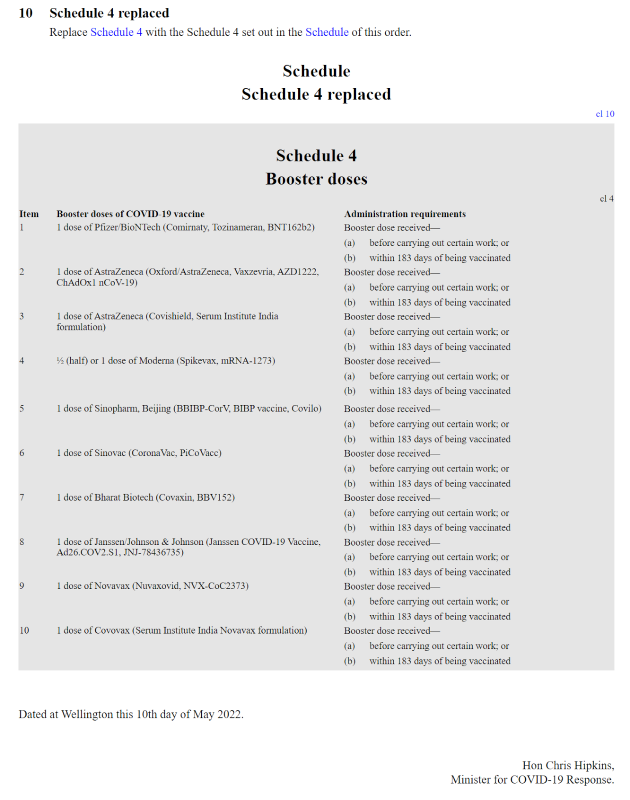
We can see that the #NZPOL and our ‘accredited’ media are pimping community masking at the same time as the Minister for COVID-19 Response, Chris Hipkins has released secondary legislation that implies ongoing mask mandates. The May 30th COVID-19 Public Health Response (Protection Framework) Amendment Order (No 9) 2022 has formalised the exemption pass for masking rules with ‘personalised’ exemption passes.
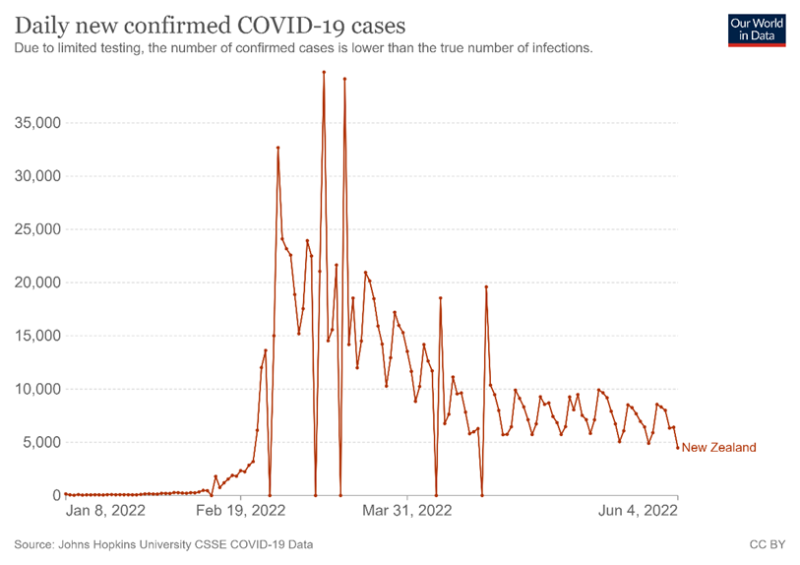
Onerous masking rules have been required by the Ardern Government for months, yet COVID-19 ripped through our secondary and tertiary institutes in February 2022, as the school year commenced. All children and young people were obliged to be fully masked up. Mask mandates in educational institutions were dropped on April 13, 2022. This unequivocal failure alone rendered the evidence for masking in a New Zealand educational context non-existent.
This graph tells a story that if anything, mandatory masking coincided with increased levels of infection in the New Zealand population.
RINSE AND REPEAT
Recent media articles promote a form of ignorance, or a culture of journalism that involves keeping nuances around real risk from COVID-19 and the role masks play (or do not play) outside the discussion.
Last week Radio New Zealand released an opinion piece stating that teachers are ‘feeling angry and unsafe because of the risk of catching Covid-19 in their classrooms.’ The pressure on students, from this article, to comply or risk being tagged as reckless, malevolent disease carriers, is alarming. It is an opinion piece because the author of the article has not discussed the evidence on the efficacy of community masking.
During April and May the media were busy with articles such as this one by microbiologist Siouxsie Wiles which promote global community masking. However, when only one study is cited as the example, which relied on modelling rather than real world data, it can be seen as ‘cherry picking.’
Wiles gets media visibility again and again. Another piece co-authored by Wiles is unable to discuss the fact that COVID-19 is not a primary risk for children and young people. It repeats the case mantra, as dogma, citing, for legitimacy, studies that only focus on transmission rates, such as this US study and this Australian study. The authors state ‘in line with other published studies’ – citing a 2020 review, long before Omicron appeared on the horizon.
While Wiles has considerable experience on bioluminescence and bacterial infections in mouse models, she is neither an expert in respiratory viruses nor an epidemiologist. There are plenty of experts in immunology and infectious diseases that remain silent.
And no, mysterious data analyst at the Ministry of Education, neither your Ministry, nor the New Zealand Government have “a responsibility to prevent as many children as possible from being infected and reinfected” with Covid-19.’
HOSPITALISATION AND DEATH
The New Zealand Government has a responsibility to keep people safe from hospitalisation and death. The Government has a duty to protect children, and consideration of well-being includes balancing the nuances. If the majority of children are not at risk from a respiratory virus, they should not have to be socially and politically coerced into wearing a (newspeak) ‘face covering’ all day, every day. And no, COVID-19 is not a far greater threat to children than the seasonal flu.
This brings the issue back to choice, and the role of masks in protecting the wearer.
Two tragedies arise from this form of cultivated, mainstream media ignorance. Firstly, such coverage, unquestioningly accepted by the general population, service workers, children and young people to daily mask wearing. These groups, who are often younger and healthier, pay the price of this cultivated ignorance in their daily ‘enmuzzlement’.
Mandates and lockdown tactics have stymied education and development. They’ve led to an increase in non-attendance. The worst taxed with remote learning have been low-income communities. Hard of hearing children have suffered immensely.
There is evidence that masks may contribute to the case fatality rate. The author theorised droplets concentrating inside masks increased exposure to the virus to the wearer, driving risk of infection.
We have never seen a bioethics panel convene to discuss such nuances – and instead, media and talking heads conflate risk with infection, over and over again.
FEAR IS NOT A PROXY FOR HEALTH
Relying on modelling can be misleading. Recently, a paper was published that claimed that mask wearing in community settings reduces SARS-CoV-2 transmission. The models remain uncertain and there is no effort to discuss the elephant, whether in Omicron the 19% reduction makes a meaningful difference.
As I have discussed, Te Pūnaha Matatini modelling for vaccine uptake excluded persistent questions of waning and breakthrough of the vaccines that might lead us to question vaccine efficacy. Our Ministries and agencies have failed to finance (at arm’s length from the institutions invested in high vaccine and mask compliance) both epidemiological studies and the literature reviews of the scientific literature on the safety and efficacy of mRNA genetic vaccines.
Modelling all too often gets put in place to legitimize predetermined policy aims. This is an utter science and governance ‘fail.’
NOPE, MASKING IN HEALTHY POPULATIONS IS NOT SETTLED
Recently when an earlier well-publicised observational CDC study was replicated, using a larger dataset and a longer time interval, the authors ‘failed to establish a relationship between school masking and pediatric cases using the same methods but a larger, more nationally diverse population over a longer interval.’
A recent study reviewing morbidity, mortality and mask usage rates across 35 countries in Europe over a 6-month period found that ‘countries with high levels of mask compliance did not perform better than those with low mask usage.’ Even in surgical settings, the effectiveness of masks remains unresolved. In the UK, in March 2022, ‘adults aged over 16 years who reported that they did not need to wear a face covering at school or work were less likely to test positive than those who reported that they always wore a face covering.’
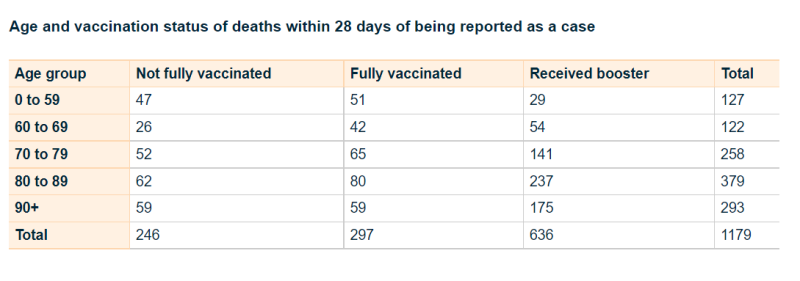
The second tragedy that can be inferred is the fear that, despite mandated vaccinations, and boosting, teachers are at risk of COVID-19. Those with multimorbidity, immunosuppressive conditions, with poorly controlled diabetes, remain at risk from SARS-CoV-2. Teachers appear to believe that masking children is the intervention that is most likely to keep them safe. And, dismayingly, it’s evident that boosted populations are now at increased risk of hospitalisation and death from COVID-19 in New Zealand.
Alarmingly, the New Zealand government has never made a space for early treatment, for nutraceutical and medical treatments that are designed to prop up the immune system; and dually reduce viral replication and risk for thrombotic events that are associated with both the SARS-CoV-2 infection, and vaccination by the mRNA genetic vaccines.
QUESTIONS MEDIA COULD ASK
If the media were acting impartially, they would ask whether there was suitable evidence that the evidence for mandates concerning the community wearing, including in educational institutions of face coverings was soundly evidence-based. Even with secondary legislation, the actual policy of mask mandates must not be arbitrary nor tyrannical.
Media would confirm that there was no way that mask wearing across the New Zealand community would be enforced in legislation, simply because there might be some indication that mask wearing prevents ‘cases.’ For it is clear from the scientific literature that most of the population is not at risk from infection, and that this has been evident from March 2020.
Such evidence would also consider the prior infection in the population, the degree to which the population has already been exposed. It would also consider the potential for harm to arise at pre-school, primary, secondary and tertiary level, from mask wearing.
Just in case the journalists of New Zealand’s government-funded media, who lack appropriate protections such as journalistic freedom of speech, are curious about these issues, I have asked the Minister in charge of this secondary legislation, the Minister for COVID-19 Response, Chris Hipkins, these very same questions.
COVID-19 EMBEDDED CONFLICTS OF INTERESTS IN GOVERNANCE
The concentration of power in relatively few hands throughout COVID-19 has placed any chance of appropriate checks and balances on the backburner.
Hipkins is also the Minister for Education. In addition to the May mask exemption legislation, Amendment Order (No 9), Hipkins has not made an effort to take meaningful measures to explain the fact why he, as the relevant Minister, would now arbitrarily pop into secondary legislation on May 15, 2022, COVID-19 Public Health Response (Vaccinations) Amendment Order (No 4) 2022. This contains a brand new schedule of outdated vaccines, that remain predominantly based on a spike protein from 2019, that now has 32 mutations. There has been no reviews of the published literature to establish, over a year after most were released, whether they are safe and effective, and work lockstep like the schedule promises, for 183 days (6 months).
The new schedule is in the form of secondary legislation. Secondary legislation does not have the checks and balances of primary legislation which include public and Parliamentary consultation.
It is evident that truckloads of secondary legislation have been churned out of the Parliamentary Counsel Office over the last few years, with no consultation with the public.
Ironically, the Member of Parliament in charge of the Secondary Legislation Bill (now Act) is the same person who sponsored the overnight legislation, the COVID-19 Public Health Response Bill that continues to be the authorising Act that gives the Labour Regime power to keep churning out the COVID-19 secondary legislation. That person is also the Attorney General, who has stated that a later amendment to that Act was perfectly fine and did not compromise the New Zealand Bill of Rights.
It is evident that the current myopic-mask media campaign aligns with recent legislation which requires mask exemptions to be digitally logged. This appears to triangulate ID systems with vaccination and contact tracing. Is this for the benefit of society, or for the benefit of digital identity schemes?
Not being able to observe the Fourth Estate acting with impartiality, in order to parse the difference between infection from a respiratory virus, and hospitalisation and death – has been one of the many tragedies of the last two years. There is no safe space for meaningful dissent and challenging conversations in New Zealand’s legacy media.
This media are not the arbiters of truth. They are tamed and compliant, and overly-dependent on opinion-based Op-eds while lacking resources, media freedom guidelines, and a public interest culture to ensure that they sniff out hypocrisy, contradiction and the missives of power.
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.