
In 2015, a viral pandemic from Northeast Brazil exploded into the news, supported by breathless public health alarms that Zika — a flavivirus acknowledged for decades as harmless — was now suddenly responsible for congenital microcephaly (babies with small heads; diminished intellect). WHO-aligned experts within Latin America recommended that women forgo childbirth indefinitely — possibly until a Zika vaccine’s fabrication (still unrealized). Massive panic predictably ensued.
Not a single case of human medical illness had previously been attributed to Zika — a near twin of the dengue virus (which itself brings a million South American “bone-break fever” cases, yearly) – – and never with any associated congenital microcephaly. Brazil’s medical research establishment treated the Zika- (and later microcephaly-) claims with initial skepticism — but were twice overwhelmed by vested parties’ self-serving media leaks – the latter of which spiraled into full-fledged national panic.
The upheavals from Zika-microcephaly included outsized public health overreactions: travel advisories; Brazilian soldiers on the streets; indelible fear; emergency injunctions proposed for abortion; the eternal absence of more than 100,000 “ghosted” Brazilian children (babies not conceived during the panic).
- “Oh, it’s bordering on the panic state for pregnant women. Wealthier women moved further south. Here, women:
- are worried whether they can get pregnant;
- use additional (layers of clothing), hoping not to be affected;
- (slather insect repellent) which … may generate another problem.”
Fortunately, the Zika pandemic has fizzled out inconspicuously and unceremoniously; never fulfilling the analysts’ predictions of an additional million microcephalic births yearly, worldwide. Nonetheless, its complete disappearance hasn’t resulted in a single scientist questioning the credibility of the underlying (likely false) premise: that receiving a Zika-carrying Aedes aegypti mosquito-bite early in pregnancy may irrevocably damage the cherished life within.
Zika, discovered in Uganda in 1947, had warranted literally only a baker’s dozen of scholarly articles in 60 years, none of which verified any human danger. In 2007, there was a bit of a “buzz” as certain dengue cases in the Pacific were relabeled by the CDC (after-the-fact and without clinical correlation) as Zika.
Zika in Bahia
In 2015, the Zika virus had heretofore never appeared in the Americas. Routine clinical Zika testing was nowhere available until many months after the announcement of the Brazilian pandemic. Most physicians and the entire public had never heard of it. Yet, despite (or perhaps because of) Zika’s void of prior significance, it became the unlikely prize within an ulteriorly-motivated medical treasure hunt. To physicians hunting, a priori, for a virus to affect social change Zika represented the clay — through wishes and partial perceptions molded into full-bore actionable fear.
In 2014, physicians Carlos Brito (of Recife) and Kleber Luz (of Natal) had formed a WhatsApp group with the literally expressed purpose of announcing a brand-new virus within Brazil; the discovery of which would address Brazil’s [poor North/wealthier South] societal inequities by bringing money and attention to Brazil’s Northeast equatorial areas. They called it “CHIKV, The Mission” – referencing both their target “chikungunya” (aka “CHIKV”, an African virus potentially making inroads into Feira de Santana, Bahia-Brazil at the time), and the 1986 movie, The Mission – in which the doctors’ anti-establishment heroes self-sacrificed in battle against the ills of European colonialism perpetrated upon indigenous populations. Ultimately, they pivoted to Zika — which served their original purpose of creating a crisis to drive increased funding even more grandly.
Dr. Luz lost the race for being the first to “unearth” Zika in Brazil, but not for lack of trying. He gave dengue patients’ serum to Dr. Claudia Duarte dos Santos, imploring her: “It’s Zika. Find Zika!” She couldn’t and didn’t – so his “Mission” was preempted in April 2015 by researchers Drs. Silvia Sardi and Gubio Soares Campos (“S&SC”) in Bahia instead.
Drs. S&SC, likely CHIKV- members themselves, similarly attributed Zika to mild dengue patients and others with achiness and rash. S&SC did so without clinical confirmation on any specific patient. The Zika PCR-test’s primer that S&SC used in their lab was a Senegalese researcher’s leftover, unverified by Brazil’s “FDA” or other researchers for efficacy. Zika and dengue are physically and genomically nearly identical, thus cross-reactive in the lab.
There was pushback to S&SC’s claim from institutional researchers who pointed out fatal flaws in S&SC’s Zika claims. S&SC responded not with the appropriate professional patience of transparently sharing their data, materials and methods for effective peer review, but by simply leaking their unsubstantiated claim directly to the popular press. This predictably created a Zika creation myth that took on its own life, independent of review, and generated a massive shockwave of panic.
Dr. Soares Campos justified his action: “We decided to benefit the public more, rather than immediately writing a scientific paper and publishing it”– as if there had been some ongoing public health emergency, while undercutting his own rationale, acknowledging “Zika is not as serious as dengue or chikungunya. The treatment is Tylenol.” Absent any pressing health dangers, why subvert the scientific process?
Bahia-State’s health ministry (SESAB) contemporaneously and publicly contradicted S&SC with a statement that the “diagnosis of Zika cases in Bahia may be wrong.” SESAB overturned half of S&SC’s results leaving only 12% of the 24 patients’ blood samples showing Zika (literally four individuals in a city of 300,000) — and any or all of those four may have been either dengue misdiagnosed, or nothing at all.
It’s debatable whether Dr. Soares Campos was able to “benefit the public more” than himself– given his professional advancement from Bahia to Buenos Aires as the self-proclaimed, “Discoverer of the Zika virus in Brazil.” His wife, Dr. Silvia, acknowledged, “We went from being two big nobodies to media stars.” Meanwhile, SESAB’s counterclaims have fallen by the wayside– no surprise as “falsehood flies, and truth comes limping after it.”
Microcephaly in Recife
Completely independently, a few months later, microcephaly was declared by neuro-pediatricians in Recife to be “epidemic” in the total absence of institutional protocol or comparison to baseline data. Stipulating their motives as honorable, believing there were more such babies in their wards – nonetheless, their methods and pronouncements were precipitous and rash. Coordinating their own physician cohorts’ WhatsApp conversations and visits to the ten local public hospitals, Drs. Vanessa and Ana van der Linden aggregated around 20 apparent cases.
In 2015, Brazil had a lax way of determining which infant had microcephaly and which had not. Brazil declared microcephaly if the infant’s head circumference was two standard-deviations below the mean – which resulted in a microcephaly diagnosis for around one out of forty births, regardless of clinical correlation. This was 17 times looser than WHO’s cutoff of three standard deviations below the mean, which meant that microcephaly was an incredibly rare finding in countries that followed the WHO standard.
Inevitably, Brazil’s overly broad criteria led to a massive overcounting of babies with physically small heads, but who were intellectually normal, as being microcephalic. This fueled the Recife doctors’ perceptions. Directly as a result of the Recife doctors’ declared microcephaly epidemic, Brazil’s nonconforming standard was twice adjusted to become appropriately stringent, and ultimately aligned with international standards.
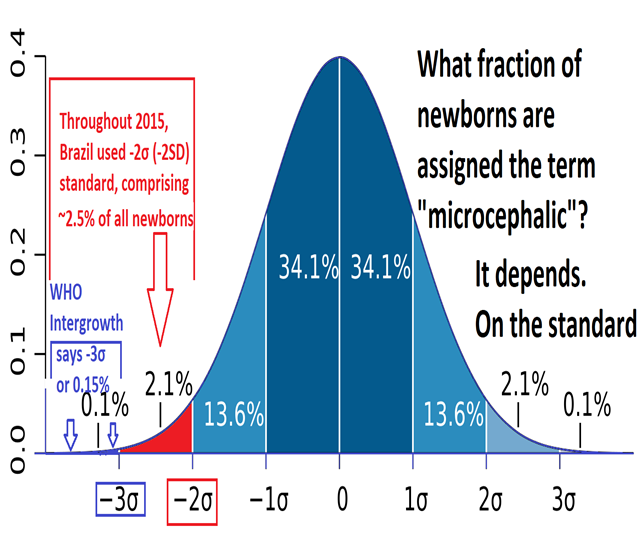
Metropolitan Recife’s population of 4 million yields ~40,000 births annually (~100 daily), from which the erstwhile standard defined 2.5% as “microcephaly,” around two such births per day. The normal neonate’s hospital stay in Brazil is two days, but longer for this diagnosis, therefore around ten such cases might at any moment reside in-hospital normally throughout Recife. This comports with the neuropediatricians’ observation and explains their alarm:
Dr. Ana van der Linden stated, “We have 3 wards (of ~7 beds each)… almost filled with children with microcephaly.” Debora Diniz continues, “The doctors had originally expected the clinic to receive ten infants [but got double; so, as a result…] Drs. Ana and Vanessa van der Linden were both certain that a new infectious disease was on the loose.”
The Zika-Microcephaly Connection
At this point, “the plot thickens.” To evaluate Recife’s microcephaly situation and the neuro-pediatricians’ premonitions, Brazil’s Ministry of Health decided on Dr. Brito, notably already invested in the notion of a newly-dangerous Zika virus:
“Dr. Brito tried to persuade his fellow epidemiologists that the microcephaly was not a product of previous underreporting or some genetic factor. He believed they were witnessing a change in an epidemiological pattern, and the cause was the Zika virus.”
With conclusion in hand, all that was needed was evidence.
Dr. Brito focused (only) on 26 mothers of microcephalic babies: asking each retroactively about rash, fever or ache 6-8 months prior. For him, an affirmative answer qualified that case as “Zika” — even with no serologic testing performed on the mothers or infants, and no control group of normal babies’ mothers given a “rash, fever, aches” questionnaire. This approach violated every basic principle of epidemiology.
Dr. Brito’s techniques, overall, were not consistent with the scientific method, involving
- “selection bias” (querying only microcephalics’ and not normal babies’ mothers)
- “lack of blinding” (eliminating the buffer layer between researcher and subject; influencing answers given to please the authoritative questioner);
- “observer bias” (the researcher’s shading answers towards his own predilection); and,
- “recall bias” (assuming accuracy of the mothers’ distant recollections)
Dr. Brito’s unsubstantiated conclusion of a novel Zika-microcephaly connection, which had been his predetermined outcome, was leaked directly to the press, subverting peer review and contemporaneous institutional replication or validation – very much redolent of S&SC’s modus operandi.
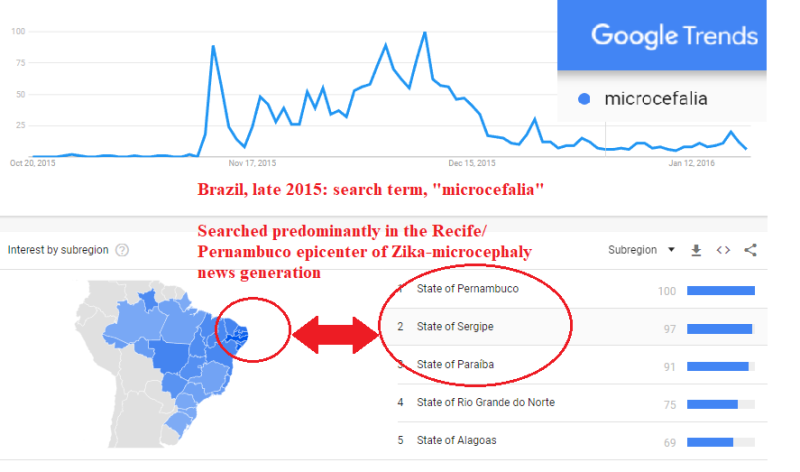
S&SC’s Zika-discovery leak garnered media attention, but absent public health ramifications soon died down. The Brito Zika-microcephaly press leak, on the other hand, communicated imminent danger and quickly cascaded into a regional, then national, then worldwide panic – the latter partially augmented by the coincidence of elites’ travel worries regarding the Rio Olympics.Confirmed cases of Zika-related microcephaly ultimately comprised fewer than 5% of the original panic-era claims. Brazil’s physicians vastly overdiagnosed neonates – from some combination of panic, overcaution, and Brazil’s incorrect and inconsistent microcephaly standards at the time. Microcephaly (as claimed) concentrated in and coincided with the location and timing of the news-generated panic (in Recife and Brazil’s Northeast) rather than with the vector-mosquito’s own range.
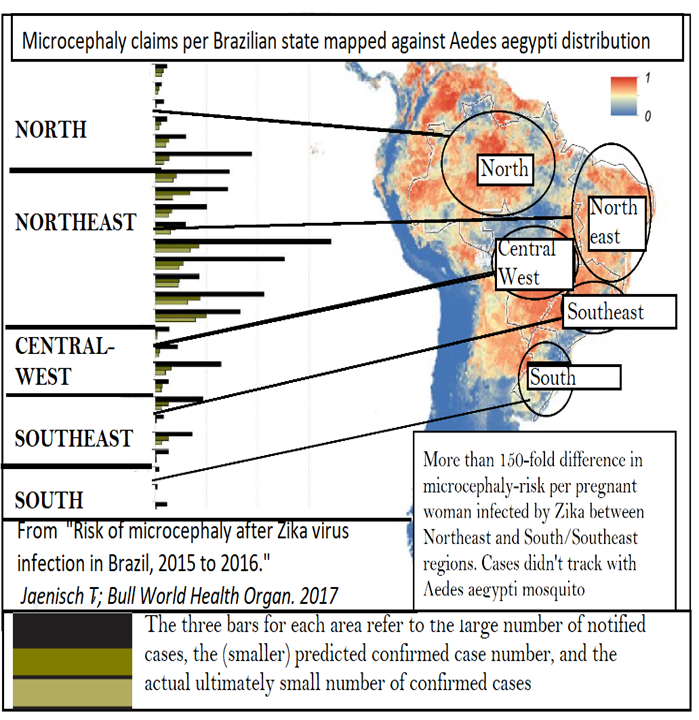
Conversely, dengue’s cases coincide geographically with this same mosquito vector, Aedes aegypti:
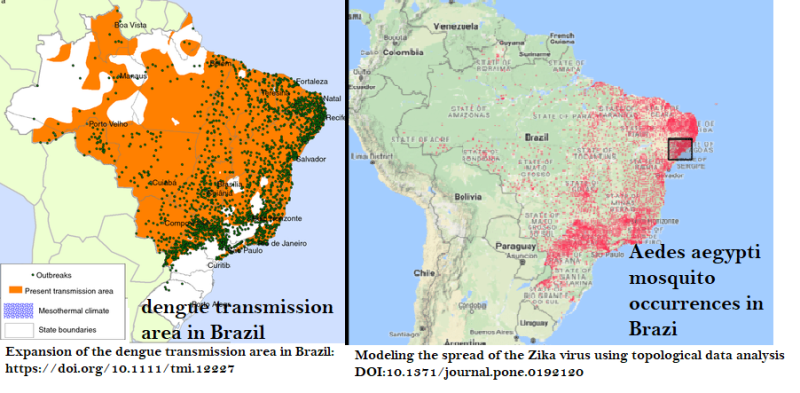
In short, dengue illness’ map overlaps with the Aedes aegypti mosquito’s distribution; while Zika-microcephaly claims were strongest where people were talking most about Zika-microcephaly.
The following year when microcephaly standards had been firmed up, and Zika diagnoses could be confirmed via proper laboratory tests, there was no further increase in microcephaly seen anywhere in Brazil including the “Ground Zero” of Recife.
Scientists are bewildered
Neither the Aedes aegypti mosquito nor its transported virus recognize national borders; yet there never was a microcephaly-rate explosion in Colombia.
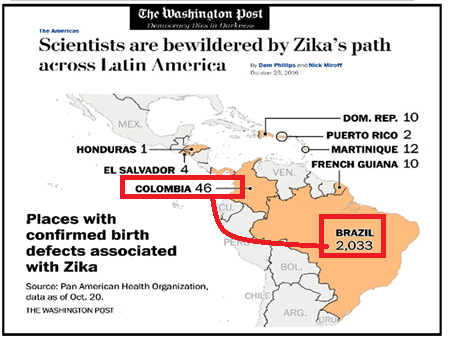
“Zika has left a puzzling and distinctly uneven pattern of damage across the Americas. To the great bewilderment of scientists, the epidemic has not produced the wave of fetal deformities so widely feared when the images of misshapen infants first emerged from Brazil.
Should we be surprised that Zika-scientists were “bewildered” by this anomaly? Add in the skepticism and suspicion science ordinarily deserves (and undoubtedly this article will garner) and the “bewilderment” disappears.
Even in Recife itself, there were vastly differing rates of microcephaly occurrence, with certain neighborhoods at orders of magnitude more than others. Wealthy neighborhoods didn’t exhibit microcephaly even though there had been no prior reason to have been overly cautious regarding mosquitoes. Arguably, the wealthy have better mosquito nets and drier streets – but they also maintain better hygiene, on average, regarding microcephaly’s pre-existing associations.
Microcephaly — aside from one severe, rare, genetically recessive “primary” version had never had a predominantly identifiable individual cause. Rather it’s a physical and statistical quantification medically characterized causally as “multifactorial,” i.e. loosely connected to a myriad of potential agents (most of which [underlined] coincide with poverty).
Disruptive injuries; Infections: “TORCHES” (toxoplasmosis, rubella, cytomegalovirus, herpes varicella, syphilis) and HIV; Poorly controlled maternal diabetes; Deprivation; Maternal hypothyroidism; Maternal folate deficiency; Maternal malnutrition; Alcohol-overuse; Teratogens: hydantoin, radiation; Maternal phenylketonuria; Placental insufficiency; Death of a monozygous twin; Ischemic or Hemorrhagic stroke
Compare this to rubella virus and its attendant congenital neurologic deformities (“rubella syndrome”) which comprise a defined cause-effect relationship. Rubella infection during a susceptible mother’s first trimester essentially always (80% -100%) brings on the syndrome; conversely the syndrome’s classic features have no other cause. Zika, once the dust had settled, was surmised to have brought (at its height) only a ~4% microcephaly-rate from its first-trimester infections.
The confluence of Zika’s low damage-rate with microcephaly’s rarity, lack of uniform presentation, and pre-existing ~twenty other loosely associative factors thwart statistical proof of causality. Imagine looking out on a field, presuming to fathom the reason for a few extra three-leaf clovers.
A Brazilian national fund began to award stipends to mothers of Zika-microcephalic babies. Even with this financial incentive newly on board, microcephaly cases associated with Zika disappeared!
In 2016 and 2017 with the advent of actual clinical Zika tests; corrected microcephaly standards; and maximal public awareness, Zika-attributed microcephaly immediately disappeared as a phenomenon. It didn’t recur in hotspot Northeast Brazil nor anywhere else on the globe. Zika showed up, for instance, in 2018 in Rajasthan India – but without attendant microcephaly.
Three Studies Reinforce Zika-Skepticism
The First:
Dr. da Silva Mattos’ “Microcephaly in north-east Brazil: a retrospective study on neonates born between 2012 and 2015” retroactively fills in the prior-year comparison data unavailable to the Recife neuropediatricians. Data-reconstruction casts doubt that there was any genuine increase in microcephaly in 2015, the year of the outbreak. The result is surprising:
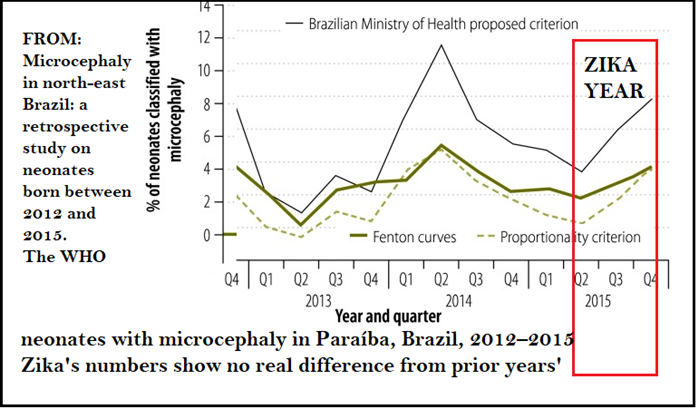
In Paraíba State (Recife/Pernambuco’s immediate neighbor to the north), the Zika panic year’s microcephaly-rate revealed itself as essentially equivalent to the newly-discovered baseline (2013 and 2014).
The Second:
Amidst the Zika outbreak uproar in late 2015, Brazil formed its “Microcephaly Epidemic Research Group” (MERG) which aimed to replicate scientifically the Drs. van der Linden and Brito examination process: focusing on the same city, Recife – but one year later. In contrast with the earlier effort this study had:
- no panic, no overdiagnosis, and no flooding the zone with alarmed moms;
- laboratory tests for Zika (and dengue);
- a control group;
- a single microcephaly standard (although still the incorrect one, 17 times too loose);
- organized and adjudicated research teams;
- no press leaks.
Remaining weaknesses were these:
- no correlation of head size with actual cognitive abilities;
- and the continuing near-impossibility of differentiating Zika from dengue.
In their own words: “Laboratory confirmation of ZIKV infection during pregnancy is challenging due to cross-reactivity with other flaviviruses, especially dengue. The neutralization test, which is the gold standard to discriminate between these viruses, is time-consuming, performed in few laboratories and does not define the time when the infection occurred.”
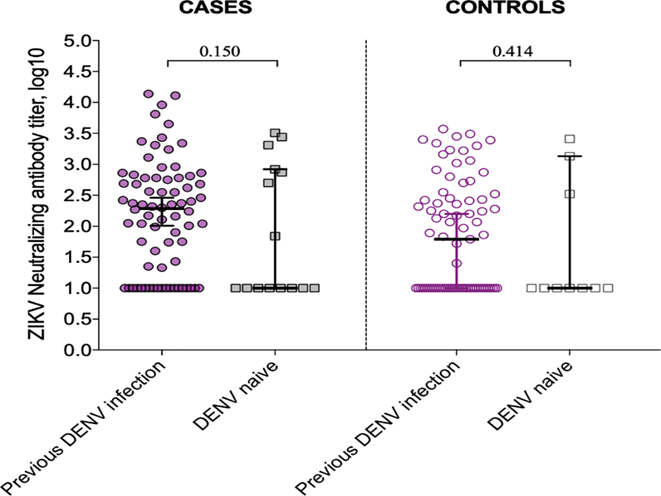
Between these two groups (of 89 mothers of microcephalics, “CASES”– and 173 moms of normal-sized babies, “CONTROLS”), there seems no gross difference in background rates of Zika-antibodies or dengue exposure. This undercuts Zika as a defining element in microcephaly.
The Third:
An analysis in central Brazil, far from media-generated panic, showed microcephaly (after Zika exposure) at such low rates as to be in line with the world’s baseline, pre-Zika.
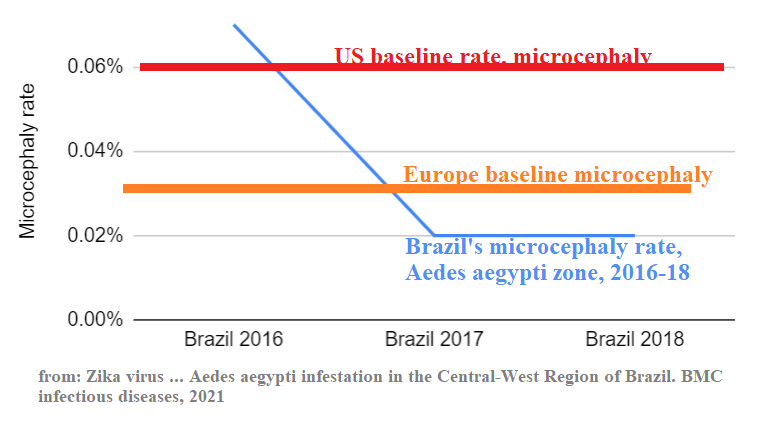
Furthermore, two years of quiet on the Zika newsfront somehow rendered the virus 3.5 times less congenitally dangerous. Is this dispositive, indicating the real viral danger was self-serving aggrandized panic?
None of these three studies emphasizes (as here) the aspects of their data bringing doubt to the Zika-microcephaly theory. None have been widely broadcast to the public, nor framed within the scientific academy so as to force reconsideration of the mass panic promulgated by folks in white coats.
Excuses, Excuses, Excuses
“There is an age-old adage, ‘If the facts don’t fit the theory, change the theory.’ But too often it’s easier to keep the theory and change the facts.” Albert Einstein
Zika-microcephaly’s proponents, in the face of reality’s capsizing their leaked predictions, have done a bit of each. Here are some of the theorized retrofits:
- Zika now, instead, causes diffuse neurologic disturbances, labeled “CZS,” Congenital Zika Syndrome.
- “Now we have tests for Zika virus … and [with microcephaly’s disappearance] we have Congenital Zika Syndrome.” Dr. Lavínia Schüler-Faccini
- One year’s exposure brought immediate Zika herd immunity to Brazil’s entire population.
- Brazil had a particularly dangerous “mutant strain.”
- The public health effort reversed Zika via awareness and avoidance.
- Dr. Ernesto Marques, epidemiologist, University of Pittsburgh
- “It could be that things associated with poverty in some way facilitate the virus to cross the placenta.”
- “Now we’ve settled on Zika as the smoking gun, but we don’t know who pulled the trigger. We suspect the villain has an accomplice, but we don’t know who it is.”
- Epidemiology Chair at Yale School of Public Health, Dr. Albert Ko suggested:
- “Are (Asian) Indians and Thais less susceptible, or are we just not detecting it?”
- “My suspicion is there is transmission, but it’s not hitting the books, it’s not being detected.”
- “Is congenital Zika syndrome being misdiagnosed as something like toxoplasmosis?”
- Was a mysterious “cofactor” of “prior exposure to dengue (enhancing) the risk of birth defects from Zika?”
- “Misdiagnosis is a reasonable hypothesis. But it’s not clear that this explanation accounts for the whole story. Zika might not be working alone.“
- “Maybe another infection combines with Zika to make the disease worse and increase the risk of birth defects.”
- Christopher Dye of the WHO admitted:
- “We apparently saw a lot of cases of Zika virus in 2016. But there was no microcephaly. The difference (between 2015 and 2016) is spectacular. First off, health officials could have vastly overestimated the number of Zika cases in Brazil. So chikungunya can easily be mistaken for Zika” … [to which NPR, to its credit, blithely responds: “But chikungunya doesn’t cause microcephaly.”]
- “There are estimated to be larger outbreaks of Zika ~ every 10 years. As Zika-naive birth cohorts age, they will become the susceptible population.” Dr. Anna Durbin
All of the above amounts to “the dog ate my homework.” None of these really hold water considering that every other tropical country also avoided the Zika-microcephaly correlation, notwithstanding an absence of herd immunity to Zika in general or any “mutant strain” in particular. None had public health campaigns comparable to Brazil’s.
The scientific backing for CZS is weak, as per the NEJM-published study often referenced. Half of the 345 women studied through 2016 tested positive for Zika during pregnancy – but ultimately produced only one case of disproportionate microcephaly unrelated to a concurrent, fetal growth restriction. The researchers, perhaps disappointed, then refocused their attention on broad but nonspecific neurologic findings – and provided this disclaimer (of observer- and selection- bias violations): “Our results should be interpreted with caution since they reflect individual neurologic assessments performed … with (prior) knowledge of in utero ZIKV infection status.”
Research funding, once turned “on,” is targeted to be kept “on” by the researchers themselves. No one admits errors. Obviously, there will be no retractions, no reformulations, despite the massive ABSENCE of further supporting data. In fact, the opposite may be occurring: doubling down.
A Missing Virus for A Missing Pandemic
Governmental response to Covid-19 provided a template of centralizing power through a public health inversion of many of its earlier precepts: e.g. emphasizing vaccines even after the relevant virus’ exit from the scene. The union of pharmaceutical companies’ financial force with public health’s sovereign power of commissioning and mandating a vaccine, while absolving its liability certainly is mutually beneficial to these stakeholders. NIAID’s forging ahead with a vaccine for Zika despite its 6-year quiescence suggests a similar temptation.
The United States Congress approved Mr. Obama’s $1 billion Zika-funding request in September 2016 (by which time, Zika-microcephaly had already shown signs of being a mirage – and Congress should have known better). About 40%, $400 million, was earmarked for production of a Zika vaccine. In the interim, a dengue vaccine has come to be, so the technology exists to produce one for Zika.
The delaying problem is nearly a Catch-22. To prove the vaccine’s efficacy, the virus has to be circulating (and dangerous in the first place, so as to warrant the effort and potential side effects). When the virus doesn’t perform its intended role of pervasiveness and danger, there’s nobody upon whom to test the vaccine and no rationale for having one to begin with.
With Zika having fizzled worldwide, and the US government’s own ethics panels having forbidden injecting and infecting people with Zika in pursuit of a vaccine, what was NIAID to do with $100 million still in hand and multiple researchers to keep employed?
In 2018, researchers attempted to circumvent the “problem” of Zika’s absence by promoting a Zika human challenge trial. This meant infecting healthy Brazilian subjects with a virus that had stopped infecting people. Johns Hopkins’ Dr. Anna Durbin revealed that Brazil’s version of the FDA had refused to [allow the United States to] conduct such experiments [on Brazilian soil]. For that reason, she set out to conduct such an experiment stateside.
Currently, paid volunteers in Baltimore are being injected with Zika – and no doubt soon enough we will have a Zika vaccine. Will this entail a Zika-vaccine mandate throughout the tropics – and, if so, cui bono? Herein lies any conspiracy theorist’s presumed impediment to a re-examination and repeal of the theory. Zika-microcephaly represents a universally accepted “emergency;” albeit one whose (hugely) major benefit to the pharmaceutical/public health -axis has not yet fully been extracted. Annulment of the theory eliminates a pharmaceutical pathway to profit and a public health pulpit.
Overturning Zika
Zika may not be the biggest news anymore, but warnings about outdoor exposure are still given to prospective mothers in the United States and elsewhere around the world. It should be removed as a concept.
The WHO, the CDC, health experts and epidemiologists are potentially effective during valid emergencies, but less so in acknowledging or self-correcting mistakes, after-the-fact. Mandates can be declared, but their fullest adoption requires genuine popular trust. There have been literally thousands of articles written on Zika, post-2015, and none, other than my Investigating Zika-Microcephaly’s ‘Crash’ in The American Journal of Medicine, questions the underlying premises or the total absence of real scientific data.
“SCIENCE” can be defined both as a body of knowledge, AND the refined, reproducible process of collecting and confirming that knowledge. Thus “questioning science” IS “science.” Science has no official “court” to determine rulings; rather (at least, in a pre-Covid-19 world) a free and open discussion mostly through journal articles. Science ultimately won’t do well or be trusted if it embodies aspects more of a priesthood than a robust, free debate.
From abrupt start to indistinct finish, the Zika-microcephaly story is rife with instances wherein the scientific method was not followed or respected. The dual episodes of “science by press leak” recalls the “cold fusion” debacle. At least in that instance, the press recovered and re-examined.
Media leaks of conjecture led to panic and compromised the timing and ability to gather adequate data to adjudicate the Zika-microcephaly hypothesis. The conjurers of Zika-microcephaly did not “benefit the public more” by cavalierly avoiding “immediately writing a scientific paper and publishing it.” Their self-aggrandizing choices handicapped concurrent experimentation, amidst a declared pandemic.
The Zika-microcephaly saga intertwines the romantic public image of intrepid, mission-driven physicians and researchers, with the reality of compromised data and active subversion of science. The Zika story has the excitement of the 1996 movie Twister, which glorifies such field researchers. In this case however, Brazil’s adventurers will ultimately have harmed more than helped: creating their own figurative ‘tornado’ whose damage through misinformation exceeded that from the mosquito’s virus.
Overturning Zika constitutes a reprieve for hundreds of millions of young women and families throughout the tropics, who need the Zika-microcephaly case not to be forgotten or papered over, but to be publicly readjudicated – but this time with the proper scientific precepts in place, and the ability to question The Emperor’s New Clothes.
There has never been a time in the history of mankind wherein a larger global audience have the words “virus,” “pandemic,” “WHO,” and “Fauci” front and center in their minds. The two pandemics are very different, but study and reexamination of Zika-microcephaly provides a more thorough and nearly complete “business case” of what can and did go wrong when scientific reviews are short-circuited.
Here are the four principal Zika conjectures, all of which need to hold true for the Zika-microcephaly connection to have been real.
- That certain, completely-untested cases essentially synonymous with dengue, showing up in dengue-endemic areas were instead and definitely (a never-before-seen-in-Brazil) Zika.
- That this Zika, previously eternally harmless to humans, had a heretofore unobserved dark side of congenital microcephaly that its twin, dengue, had never exhibited, and just as quickly simply vanished.
- That claiming more microcephaly (without prior data-comparison) in one area of Brazil (Recife, during a panic) implied a significant nationwide increase (throughout Aedes aegypti’s entire territory).
- And that one completely novel, scientifically-unverified, laboratory-unmeasured improbability (Zika) had caused the other (microcephaly).
“It was my understanding that there would be no math.” — Chevy Chase
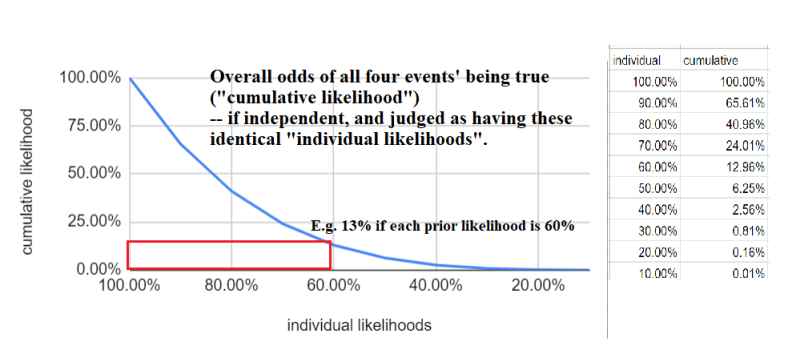
Not too much is needed here; simple probability theory suffices. If, for instance, we place a likelihood of each of these independent conjectures at 30%, then the likelihood all four are correct is ~1%. Ultimately the greater surprise is not Zika-microcephaly’s disappearance, but its quick acceptance as scientific dogma; with the lesser surprise that it has been left to this “outsider” general practice physician to document these issues.
Meanwhile Zika theorizers in the scientific academy can take solace in fictional detective Hercule Poirot’s self-confidence: “Always I am right. It is so invariable it startles me. And now it looks very much as though I may be wrong, and that upsets me. But I should not be upset, because I am right. I must be right because I am never wrong.”
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








