
I dedicate this article to all women invited to mammography screening and those who love them because the public has consistently been lied to, for over 40 years. In invitations to screening, women have been told that by detecting cancers early, screening saves lives and leads to less invasive surgery.1,2 I shall demonstrate that all three statements are wrong.
Women are still being told these lies, by professional associations, screening advocates, screening researchers, cancer charities, and national boards of health.3-5 The American Cancer Society declares in a headline that “Mammography Saves Lives”4 and claims, with no references, that results from many decades of research clearly show that women who have regular mammograms are less likely to need aggressive treatments like surgery to remove the entire breast (mastectomy).5
Screening Does Not Save Lives
In the randomised trials of mammography screening, the risk ratio for overall mortality after 13 years of follow-up was 0.99 (95% confidence interval 0.93 to 1.03) for those trials with adequate randomisation.6 The estimate happened to be the same for the other trials, some of which were so poorly randomised that the average age in the two compared groups was not the same, which makes an analysis of overall mortality unreliable.
For two of the three adequately randomised trials, those from Canada and the UK, there are follow-up data after 25 and 23 years, respectively.7,8 The risk ratio for overall mortality was 1.01 (95% confidence interval 0.98 to 1.03) for all three trials (both with a fixed effect and a random effects model, Comprehensive Meta Analysis Version 3.0). In the table, the year means the year the trial started:
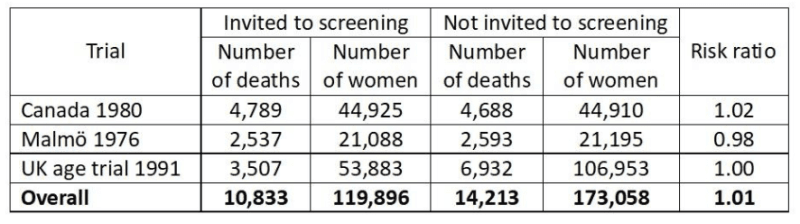
This is a very strong result as it is derived from a total of 25,046 deaths. We can therefore say with great confidence that mammography screening does not save lives.
If we restrict the analysis to the two trials with a very long follow-up, the result is the same, a risk ratio of 1.01 (0.99 to 1.04).
Breast Cancer Mortality Is a Seriously Flawed Outcome
It will surprise most people to learn that we cannot trust what has been reported in the randomised trials about the effect of screening on breast cancer mortality but this is an objective fact.6
A minority of the women who died were autopsied, and in several trials, cause of death was not assessed blindly.6 I have documented that assessment of cause of death was seriously biased.6,9 If we include all trials in the analysis, we would expect to see the greatest reduction in breast cancer mortality in those trials that were most effective in lowering the rate of node-positive cancers (cancers that had metastasised) in the screened group.
This was indeed the case, but the regression line was in the wrong place. It predicts that a screening effectiveness of zero (i.e. the rate of node-positive cancers is the same in the screened groups as in the control groups) results in a 16% reduction in breast cancer mortality (95% confidence interval 9% to 23% reduction).6,9 This can only happen if there is bias, and further analyses showed that assessment of cause of death and of the number of cancers in advanced stages were both biased in favour of screening.
Systematic reviews that include all the trials, also the poorly randomised ones, have reported that mammography screening reduces breast cancer mortality by 16-19%.6,10 As this estimate is of the same size as the bias in the regression analysis, this suggests that screening does not lower breast cancer mortality.
Another reason why breast cancer mortality is a flawed outcome is that screening leads to overdiagnosis, which is the detection of cancers and precursors to cancer (carcinoma in situ), which would not have come to the attention of the woman in her remaining lifetime and therefore would not have become a problem without screening. Since it is not possible to distinguish between harmless cancers and dangerous ones, they are all treated, and radiotherapy and chemotherapy given to women who are healthy increase their mortality.6
If we take into account the cardiac and lung cancer deaths caused by the type of radiotherapy used when the screening trials were carried out and generously assume that screening reduces breast cancer mortality by 20% and results in only 20% overdiagnosis of healthy women, then there is no mortality benefit from screening.11
Finally, it is noteworthy that the most unreliable trials were those that reported the greatest reductions in breast cancer mortality.6 The difference in the effect estimates between the adequately randomised trials and the poorly conducted trials was statistically significant, both after 7 and 14 years of follow-up (P = 0.005 and P = 0.02, respectively).12
Total Cancer Mortality
Since misclassification of cause of death often concerns deaths from other cancers,6 total cancer mortality is a less biased outcome than breast cancer mortality.
Some trialists have not reported what the total cancer mortality was but we have data from the three adequately randomised trials.6,8 There was no effect of screening on total cancer mortality, including breast cancer, risk ratio 1.00, 95% confidence interval 0.96 to 1.04. There were two different age groups in the Canadian trial, 40-49 (a) and 50-59 years (b):
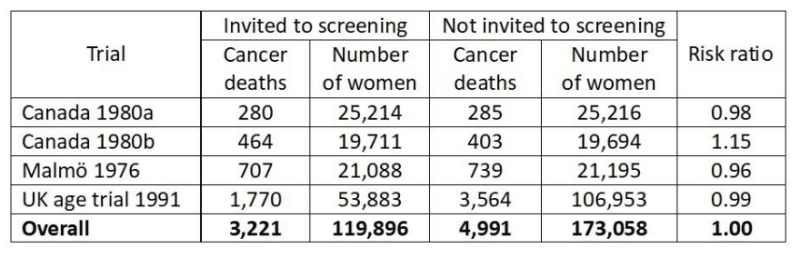
Since total cancer mortality is less biased than breast cancer mortality, it is of interest to see what the expected cancer mortality (including breast cancer mortality) would have been if the reported reduction in breast cancer mortality of 29% after 7 years in the poorly randomised trials6 were true.
It would have been a risk ratio of 0.95, which is significantly lower (P = 0.02)6 than what was actually found. This provides further evidence that assessment of cause of death was biased in favour of screening.
Breast Cancer Is Not Detected Early but Very Late
If we assume that the observed doubling times in longitudinal tumour studies are constant from initiation till the tumour becomes detectable, the average woman has harboured the cancer for 21 years before it acquires a size of 10 mm and becomes detectable on a mammogram.13
Given this large time span, it is misleading to call it “early detection” also because the effect of screening is trivial, namely to advance the diagnosis by less than a year.13
Yet all authorities repeat this mantra. As it is impossible that everyone working with cancer is unaware of the basics of tumour biology, we can draw the conclusion that the public all over the world is being misinformed. This is fraud because it is deliberate and because women think “early detection” will save their lives.
I once asked a famous tumour biologist, Keld Danø, during a coffee break at an international meeting, whether he agreed with me that it was impossible to lower breast cancer mortality by 30% with screening, based on our knowledge of tumour biology.14 He agreed. When I asked why people like him didn’t participate in the scientific debate, he didn’t reply and it is not difficult to imagine why. It is not wise to point out that your colleagues are wrong when you are on the receiving end of major funds from a cancer charity that touts screening.
The women suffer while everyone else prospers.
The earliest cell changes, carcinoma in situ, are not detected unless the women get a mammogram. In our systematic review of countries with organised screening programmes, we found an overdiagnosis of 35% for invasive cancer and 52% when we included carcinoma in situ.15
Although less than half of carcinoma in situ cases progress to invasive cancer,16,17 the women are nevertheless routinely treated with surgery, drugs, and radiotherapy.
The deep irony is that the surgery is often mastectomy because the cell changes may be diffusely spread in the breast, and sometimes even in both breasts. In New South Wales, one-third of women with carcinoma in situ had a mastectomy,18 and in the UK, carcinoma in situ was more often treated by mastectomy than invasive cancer,19 and the number of women treated by mastectomy almost doubled from 1998 to 2008.20
This brings us to the third big falsehood in the propaganda about mammography screening.
Screening Does Not Decrease but Increases Mastectomies
Because of the substantial overdiagnosis of invasive cancer and carcinoma in situ, and because screening only advances detection of invasive cancers slightly,13 it is inevitable that screening increases mastectomies.
In the randomised trials of screening, we found 31% more mastectomies in the screened groups than in the control groups.6
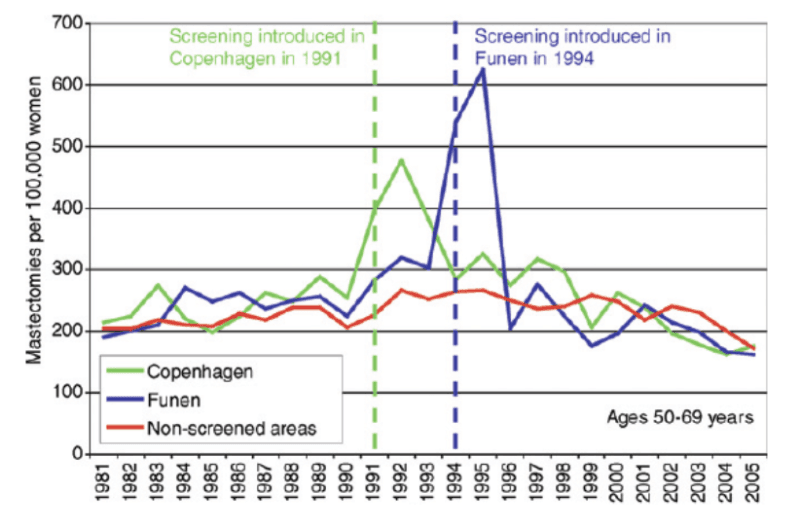
Denmark is a unique country to study this in practice as we had a period of 17 years (1991-2007) where only about 20% of potentially eligible women were invited to screening because some counties did not have screening.21 When screening starts, more breast cancer diagnoses than usual will be made and there will be more mastectomies. However, as can be seen on the graphs, the huge increases in mastectomies are not compensated by a drop in mastectomies later where there was a similar decline in mastectomies in non-screened areas as in screened areas:22
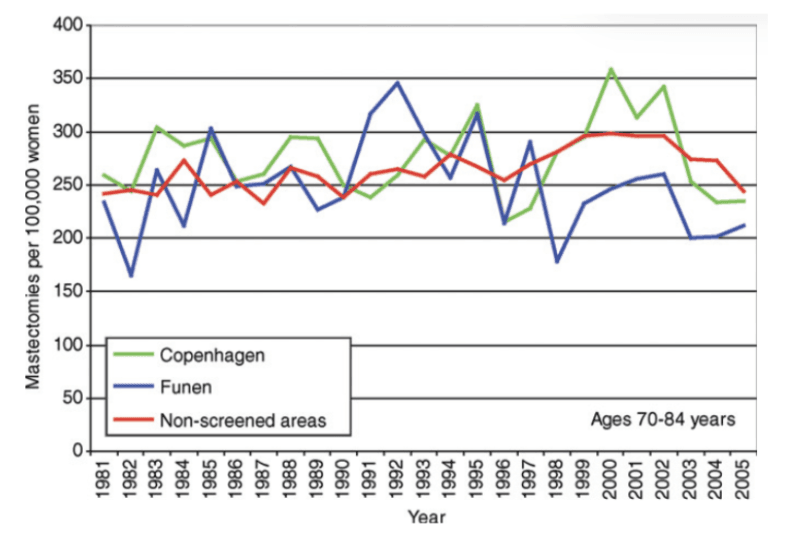
Moreover, as the next graph shows, there is no compensatory drop in old age groups:22
Yet women are told that screening leads to less invasive surgery, with fewer mastectomies. This is disinformation in the extreme.
The most commonly used trick used to disinform the women about this issue is to report percentages instead of numbers.3 Imagine a town with a certain level of crime. You divide the crimes into serious and less serious ones. Over a period of time, the rate of serious crime increases by 20% and the rate of less serious crime by 40%. This is a development for the worse. But although more people are exposed to serious crime and more people are exposed to less serious crime as well, a trickster would say that, as there are now relatively fewer cases of serious crime, the situation has improved.
It is deplorable that people who know better – screening researchers, cancer charities, national boards of health, etc – have lied to the public this way3 and still do, in direct contrast to logic and the scientific evidence.
The Final Layers of Dishonesty
The mammography screening area is riddled with dishonesty. So much that I needed to write a whole book detailing all the elaborate ways in which researchers and others had made it look like the Emperor was dressed when in fact he was naked.3
The deception is total because it always continued after I had pointed out in letters to the editor what the researchers had done wrong, and to which they responded.3,14 They therefore cannot claim they didn’t know that they continued to manipulate the data and to deceive the public.
Three of the most dishonest and most prolific authors are László Tabár, Stephen Duffy, and Robert Smith. Over many years, they aggressively attacked my extensive research on mammography screening but never with convincing arguments3,14 – they excel at ad hominem arguments.
László Tabár was the primary investigator for the Swedish Two-County study, an early trial that reported a huge effect of screening, a 31% reduction in breast cancer mortality.23 This trial was instrumental for introducing screening. However, there are so many serious discrepancies in numbers, and some of the findings are so implausible and incompatible with reported tumour characteristics, that it looks like scientific misconduct.3,6,24-27 Tabár has made a fortune on mammography screening and has a habit of threatening with litigation whenever anyone gets too close to his secrets.3,14,23
One would not think that Stephen Duffy is a professor of statistics because he has bent the data beyond belief and beyond what is appropriate in many creative and obscure ways.3,6,14 Robert Smith was once the Director of Cancer Screening at the American Cancer Society.
This triumvirate reported a 63% reduction in breast cancer mortality in an observational study.28 I pointed out some of the problems with their study,29 but in their reply,30 they
compared women who attended screening with women who didn’t, although it is clear from
their own paper that they were aware that such comparisons are seriously misleading.
These authors claimed, based on the Two-County study data, that they had found a “statistically significant 13% reduction in mortality in association with an invitation to screening.”31,32 This is plain wrong and totally impossible. Even if screening was 100% effective and prevented all deaths from breast cancer, it could not reduce total mortality by 13%.
They furthermore predicted that when a screening programme had been running for some time, one could expect a reduction of 3-4% in total mortality.31 This is also impossible unless screening prevents all breast cancer deaths. The lifetime risk of dying from breast cancer is 2.5-3%,33 and it was 3-4% in many countries before screening was introduced.
I dryly remarked in my book that if they continued their line of research for other diseases, they may find the recipe for eternal life.3 I also noted that the problem with lying is that
sooner or later people usually contradict themselves, which they did in relation to a study they had published in The Lancet.3
A common way of duping the readers is to say that early detection of breast cancer “reduces mortality”34 without specifying what kind of mortality this is, which makes the reader believe that screening saves lives.
The most common error in the screening literature could be that people falsely translate a recorded effect on mortality from a cancer into an effect on all-cause mortality. We see claims everywhere that common cancer screening tests save lives but a systematic review of the randomised trials found that the only screening test with a significant lifetime gain was sigmoidoscopy. It extended life by 110 days on average, and as the 95% confidence interval went from 0 to 274 days, this result was on the verge of not being statistically significant.35
Another common trick is to use hypothetical statements when we have certain knowledge. For example, authors may write – even in our most esteemed medical journals – that overdetection “may” occur for invasive cancers and that it “may” cause harm through unnecessary labelling and treatment of patients who, without screening, “might” never have been diagnosed.34 These are not hypothetical possibilities; they are inevitable consequences of screening.
Final Remarks
Starting in 2000, I have published numerous scientific articles, letters to the editor, newspaper articles, and two books about mammography screening that do not leave a shred of doubt that this intervention is very harmful.37
Even though I know that no one will ever be convicted, I consider it a crime that women have been systematically lured into believing that screening is good for them. According to the principles for informed consent, people must be fully informed about the most important benefits and harms of interventions they are offered, but this ethical requirement has been brutally ignored. To such a degree that in many countries, women receive an “invitation” to mammography screening with a pre-allotted time for a mammogram they never asked about.1 This makes them believe it is very important that they show up and puts pressure on them to cancel the appointment if they don’t want a mammogram taken. If they refuse, they are often subjected to highly coercive and paternalistic follow-up letters.
Here are some examples of the deeply unethical practice:1
“We have reserved a time…If the time is very inconvenient, we ask you to contact the mammography screening centre as soon as possible;” “I am concerned that you have not yet responded to our recent invitation for a screening mammogram;” “If you would like to avoid participation, we ask you to fill out a form. You obtain this form by calling the breast-diagnostic centre;” “During the past two years, over 340 000 Queensland women have benefited from taking part in the BreastScreen Queensland Programme,” “You can take a positive step to decrease your own risk, and help us achieve our goal, by deciding to take part.”
What matters is to ensure a high uptake, “our goal,” not that the women understand what they are being subjected to.
I advise women in all countries to not go to mammography screening and to do nothing if they are “invited,” which my wife did. She had no obligation to decline an “invitation” with a pre-allotted time she never asked for, and the letter made her angry.
Screening is harmful in many other ways than those I have mentioned here, e.g. between one quarter and one half, depending on the country, of all women attending screening repeatedly will experience at least one false positive result, which can be distressful for several years.36 It therefore constitutes another tremendous harm.6,14
As I have explained elsewhere,38 the Cochrane Collaboration refused to allow us to update our Cochrane review on mammography screening last year, even though I had updated it three times before and the update was only about adding more deaths to two of the trials.
Absurdly, the ”Sign-Off Editor” noted that our review might create a potentially damaging firestorm of misinformation and we were accused of having pre-conceived ideas about no benefit of screening “rather than considering it may actually have benefit not detected.” We were also forbidden to use the term overdiagnosis even though this is standard and appears in other Cochrane reviews of cancer screening, including our own.6,12
When I first published the Cochrane review, in 2001, there was a huge scandal39 because Cochrane forbade us from publishing our data on the most important harms of screening, overdiagnosis, and overtreatment.3 This should have made the Cochrane leaders handle our update professionally, but they preferred to support the prevailing dogma about screening rather than telling the women the truth.
Only one question remains: Which country will be the first to show a little sanity and respect for the science and abandon screening?
References
1 Jørgensen KJ, Gøtzsche PC. Content of invitations to publicly funded screening mammography. BMJ 2006;332:538-41.
2 Gøtzsche P, Hartling OJ, Nielsen M, Brodersen J, Jørgensen KJ. Breast screening: the facts – or maybe not. BMJ 2009;338:446-8.
3 Gøtzsche PC. Mammography screening: truth, lies and controversy. London: Radcliffe Publishing; 2012.
4 Mammography Saves Lives. American College of Radiology 2026; Feb 27.
5 American Cancer Society Recommendations for the Early Detection of Breast Cancer. 2026; Feb 27.
6 Gøtzsche PC, Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Sys Rev 2013;6:CD001877.
7 Miller AB, Wall C, Baines CJ, et al. Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial. BMJ 2014;348:g366.
8 Duffy SW, Vulkan D, Cuckle H, et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. Lancet Oncol 2020;21:1165-72.
9 Gøtzsche PC. Relation between breast cancer mortality and screening effectiveness: systematic review of the mammography trials. Dan Med Bull 2011;58:A4246.
10 Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med 2002;137(5 Part 1):347-60.
11 Baum M. Harms from breast cancer screening outweigh benefits if death caused by treatment is included. BMJ 2013;346:f385.
12 Gøtzsche PC, Nielsen M. Screening for breast cancer with mammography. Cochrane Database Syst Rev 2006;4:CD001877.
13 Gøtzsche PC, Jørgensen KJ, Zahl PH, Maehlen J. Why mammography screening has not lived up to expectations from the randomised trials. Cancer Causes Control 2012;23:15-21.
14 Gøtzsche PC. Mammography screening: the great hoax. Copenhagen: Institute for Scientific Freedom; 2024 (freely available).
15 Jørgensen KJ, Gøtzsche PC. Overdiagnosis in publicly organised mammography screening programmes: systematic review of incidence trends. BMJ 2009;339:b2587.
16 Nielsen M, Thomsen JL, Primdahl S, et al. Breast cancer and atypia among young and middle-aged women: a study of 110 medicolegal autopsies. Br J Cancer 1987;56:814-9.
17 Welch HG, Black WC. Using autopsy series to estimate the disease reservoir for ductal carcinoma in situ of the breast. Ann Intern Med 1997;127:1023-8.
18 Kricker A, Smoothy V, Armstrong B. Ductal carcinoma in situ in NSW women in 1995 to 1997. National Breast & Ovarian Cancer Centre 2000;April 15.
19 Patnick J. NHS Breast Screening Programme: annual review 2011. NHS Breast Screening Programme 2012.
20 Dixon JM. Breast screening has increased the number of mastectomies. Breast Cancer Res 2009;11(Suppl 3):S19.
21 Jørgensen KJ, Zahl P-H, Gøtzsche PC. Overdiagnosis in organised mammography screening in Denmark: a comparative study. BMC Womens Health 2009;9:36.
22 Jørgensen KJ, Keen JD, Gøtzsche PC. Is mammographic screening justifiable considering its substantial overdiagnosis rate and minor effect on mortality? Radiology 2011;260:621-7.
23 Tabár L, Fagerberg CJ, Gad A, et al. Reduction in mortality from breast cancer after mass screening with mammography. Randomised trial from the Breast Cancer Screening Working Group of the Swedish National Board of Health and Welfare. Lancet 1985;1:829-32.
24 Zahl P, Kopjar B, Mæhlen J. Mammografistudier. Tidsskr Nor Lægeforen 2001;121:2636.
25 Gøtzsche PC, Mæhlen J, Zahl PH. What is publication? Lancet 2006;368:1854–6.
26 Zahl P-H, Gøtzsche PC, Andersen JM, Mæhlen J. Results of the Two-County trial of mammography screening are not compatible with contemporaneous official Swedish breast cancer statistics. Dan Med Bull 2006;53:438-40.
27 Gøtzsche PC. Whistleblower in healthcare (autobiography). Copenhagen: Institute for Scientific Freedom 2025 (freely available).
28 Tabár L, Vitak B, Chen HH, Yen MF, Duffy SW, Smith RA. Beyond randomized controlled trials: organized mammographic screening substantially reduces breast carcinoma mortality. Cancer 2001;91:1724-31.
29 Gøtzsche PC. Beyond randomized controlled trials. Cancer 2002;94:578.
30 Tabár L, Duffy SW, Smith RA. Beyond randomized controlled trials. Authors’ reply. Cancer 2002;94:581–3.
31 Tabár L, Duffy SW, Yen MF, Warwick J, Vitak B, Chen HH, Smith RA. All-cause mortality among breast cancer patients in a screening trial: support for breast cancer mortality as an end point. J Med Screen 2002;9:159–62.
32 Duffy SW, Tabár L, Vitak B, Yen MF, Warwick J, Smith RA, Chen HH. The Swedish Two-County trial of mammographic screening: cluster randomisation and end point evaluation. Ann Oncol 2003;14:1196–8.
33 Office of Population Censuses and Surveys. Mortality Statistics: cause 1988. London: HMSO; 1990. (Series DH2 no. 15. Table 2).
34 Irwig L, Houssami N, Armstrong B, Glasziou P. Evaluating new screening tests for breast cancer. BMJ 2006;332:678-9.
35 Bretthauer M, Wieszczy P, Løberg M, et al. Estimated lifetime gained with cancer screening tests: a meta-analysis of randomized clinical trials. JAMA Intern Med 2023;183:1196-1203.
36 Brodersen J, Siersma VD. Long-term psychosocial consequences of false-positive screening mammography. Ann Fam Med 2013;11:106–15.
37 Gøtzsche PC. Mammography screening is harmful and should be abandoned. J R Soc Med 2015;108:341-5.
38 Gøtzsche PC. Cochrane on a suicide mission. Brownstone Journal 2025; June 20.
39 Horton R. Screening mammography – an overview revisited. Lancet 2001;358:1284-5.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








