
Early on in the pandemic lockdowns, I got a call from a friend in Texas. He reported that local hospitals were furloughing nurses, and the parking lot was completely empty. I didn’t believe it.
This was a pandemic. How could this be true? News was filled with reports of crowding within several hospitals in New York – even if a 1,000-bed Navy hospital was mostly used – and one had the impression that this was probably happening all over the country. It wasn’t. The problem was local and short term, but most of the country never faced a hospital capacity problem.
After hanging up the phone with my friend, I looked for news stories. Sure enough, he was right.
The nursing furloughs began and didn’t stop for another six months. Overall, 266 hospitals furloughed nurses for the spring and summer of 2020 – the very height of the pandemic.
I got curious and was amazed to find that a central plan had been imposed for the health care system, around the same time that schools were closed and events forcibly cancelled. Throughout the country, elective surgeries were either postponed or cancelled to prepare for Covid patients who weren’t there.
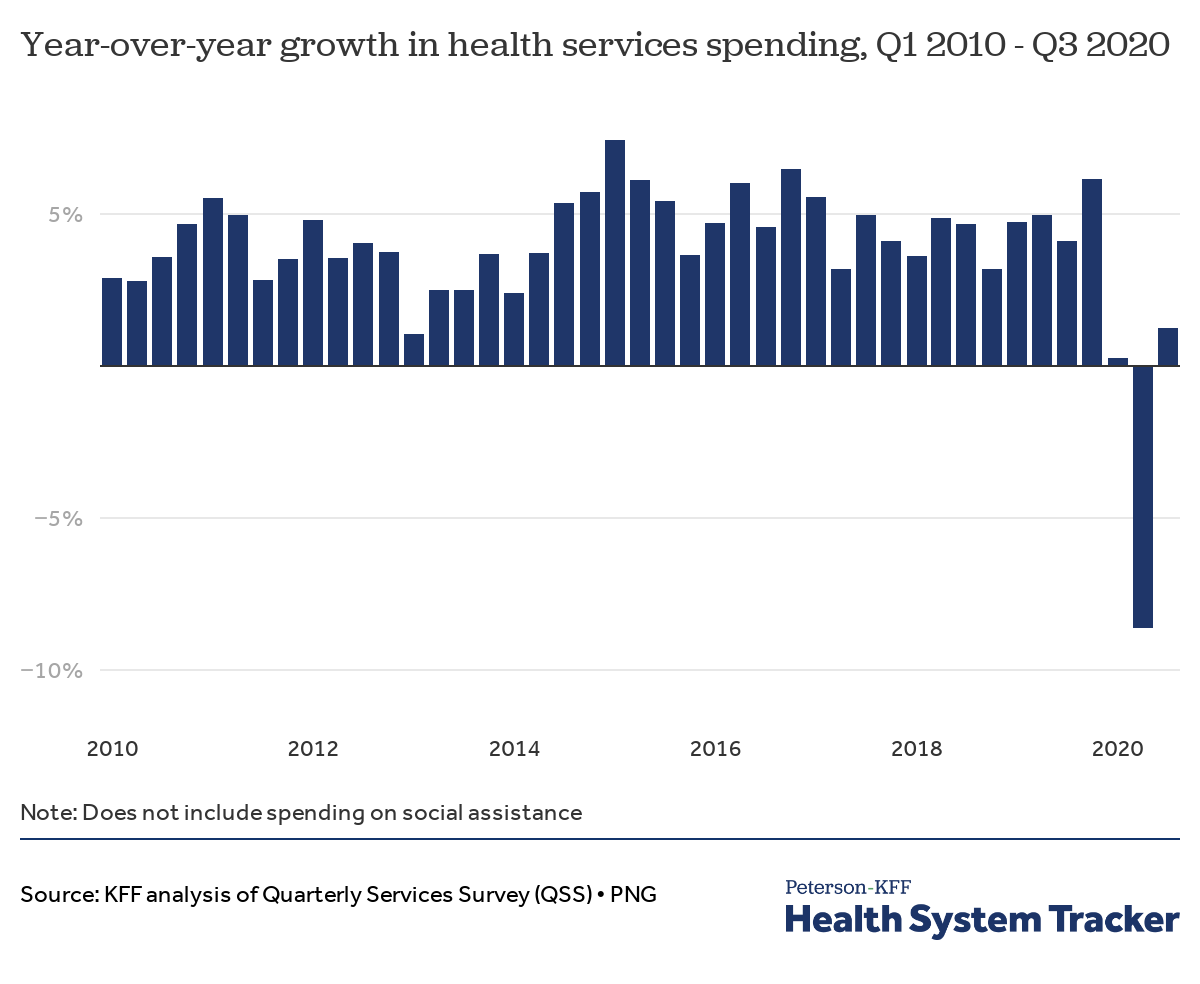
Even now, this bizarre feature of 2020 has not been widely discussed. But just check out the numbers from the second quarter as shown in this surprising chart.

The American Hospital Association estimated that the whole industry lost $202.6 billion in revenue between March and June 2020. By July, the AHA estimated the losses would be $323 billion by year’s end.
In the first half of the year, inpatient admissions fell by 20%, while outpatient visits collapsed by 35%. Visits to the emergency room crashed too, in some places by as much as 42%. By the fall of 2020, elective surgeries were down by 90% of where they would normally be.
There are millions of human tragedies buried in these numbers and you probably know of stories yourself. I certainly do.
We can speculate as to the reasons. People were afraid and didn’t want to get out for fear of Covid. Also there was a concern that no matter what services one needed, being diagnosed as Covid positive could land you in ICU where you didn’t want to be. There was also the general feeling out there that the whole medical sector had become vaguely scary and not worth approaching – exactly what one does not desire in a pandemic.
And yet there is another factor: government force. Tenet Health in July 2020 explained what happened, blaming public panic but also “government cancellation of elective surgeries and shelter-at-home requirements coupled with the mandate for all hospitals and associated support to remain fully operational.”
Consider what this means. In nearly every state, and perhaps there were exceptions I cannot seem to find, health care systems were forcibly reserved for Covid-19 patients and emergencies, and this was enforced. Even South Dakota, which otherwise had no lockdowns, briefly stopped most non-Covid services.
A typical edict read such as this one from Washington State, via the governor’s office: “I hereby prohibit all medical, dental and dental specialty facilities, practices, and practitioners in Washington State from providing non-urgent health care and dental services, procedures, and surgeries unless they act in good faith and with reasonable clinical judgment to meet and follow the procedures and criteria provided (in guidelines listed in the proclamation).”
Elective surgeries were out, and this does not mean “stuff that is not important.” It means surgeries that can be scheduled in advance. It could be a mastectomy, a hip replacement, removing kidney stones or an appendix, or any number of other services.
How did this happen? Who ordered it? Who came up with the idea in the first place, rather than simply letting hospitals and doctors make their own judgements about services? And why in the world did the people who imposed these rules not consider the likelihood that not everywhere in the country would be equally impacted by Covid at the same time?
The Fauci emails provide a clue. The first mention that I can find of the supposed need to segregate patients into non-elective and elective surgeries, Covid vs non-Covid, comes from a February 18, 2020, message by VA consultant and pandemic planner Carter Mecher, the same man who exercised such a powerful influence on shutting schools down. His outsized influence in driving the national lockdowns was apparently due to his passion, seeming knowledge, high-level access, and astonishing loquaciousness.
He wrote Fauci and others on that day as follows:
“I would anticipate that the tripwire for implementing NPIs [euphemism for lockdowns] (community transmission), will also be the trigger for healthcare systems to dial down or tum off elective admissions (primarily surgical) to free up acute care and ICU/monitored meds. The most effective way to protect these nonacute areas is by shunting potential COVID patients away from these areas and either providing this type of care while the patients is hospitalized in acute care or thru telephone care/home care for patients with mild illness receiving care at home. And the most effective way to shut these patients away from non-acute care areas is thru the implementation of early and aggressive NPis of isolation of the ill and home quarantine of household contacts.”
What’s striking here is how it came to be that one man imagined that he had sufficient knowledge of health care services, the virus trajectory, severity, geography, and other demographic factors to make such decisions. In fact, he didn’t even bother to discover such detail. He simply assumed, as central planners do, that the country is one big homogenous blob of people who need a planner at the top to tell them what to do.
And it wasn’t just health care. He had a plan for schools and, really, the entire country. On February 17, 2020, Mecher flat-out stated that lockdowns were going to be the path. This was the time when Fauci was in public claiming otherwise.
Mecher wrote: “NPIs are going to be central to our response to this outbreak (assuming our estimates of severity prove accurate)… Looking ahead, I anticipate we might encounter pushback over the implementation of NPls and would expect similar concerns/arguments as were raised back in 2006 when this strategy first emerged.”
There are still many remaining mysteries as to how all this happened, particularly as it pertained to health care. No question that terrifying models from the IHME predicted massive hospital overruns all over the country that did not actually arrive. Meanwhile, the pandemic did in fact lead to a massive health crisis (not just in the US but around the world) due to forced blockages of medical services as part of lockdown plans.
We need more research into the origins of the lockdown calamity, particularly as it affects health care. This chaos was not “driven by the pandemic” (no thank you, NYT) but by the lockdowns and attempt to run the country by executive fiat.
What lessons will be learned? Who will teach them? This is an egregious example of the utter failure of an arrogant central plan that presumed to know and act upon what in fact could not be known. It was a failed experiment with lasting consequences on millions and billions of lives.
Join the conversation:
[Sassy_Follow_Icons social_networks="x=https://x.com/brownstoneinst,facebook=https://www.facebook.com/brownstoneinst,telegram=https://t.me/brownstoneinst, truth_social=https://truthsocial.com/@brownstoneinst, linkedin=https://www.linkedin.com/company/brownstone-institute/, gettr=https://gettr.com/user/brownstoneinst, gab=https://gab.com/brownstoneinst" shape="round" style="background-color:#ac3900;]
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.









{kind=link}