In my epidemiology coursework, many years ago, I was taught that the smallpox vaccine had eradicated that dreadful disease. It was common knowledge, so I did not question the claim.
They did not tell me about favorable time trends in the natural course of other infectious diseases for which there was no vaccine, nor about the correlation of those trends with improved living conditions, sanitation, personal hygiene, and nutrition. The unexplained transition from the severe form of smallpox (variola major) to the mild form (variola minor) in the Western world was not mentioned. All the credit was given to the smallpox vaccine.
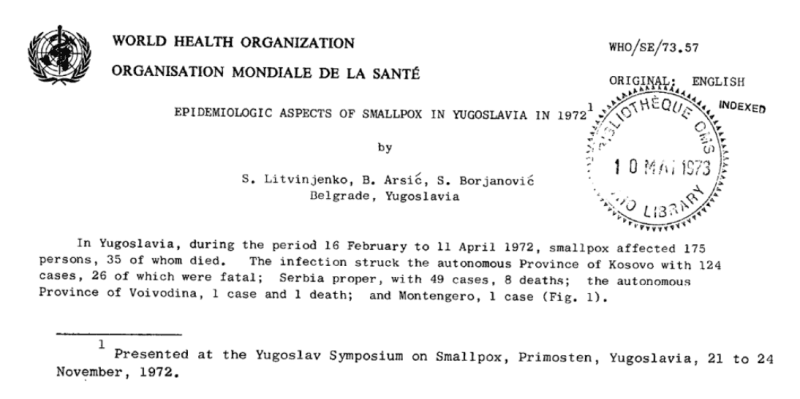
Of course, no randomized trial of that vaccine was ever conducted. There was, however, a natural experiment in Yugoslavia in 1972—a short-lived outbreak of smallpox with a total of 175 infected people and 35 deaths. Besides a vaccination campaign, there are interesting parallels to the Covid story, so it is worthwhile to re-examine that outbreak.
My primary sources were a document published by the WHO in November 1972 and a paper published 50 years later. Another recent paper also provided a historical review of the population of Kosovo, where almost three-quarters of the cases have occurred. As expected, all three papers and others attribute the end of the smallpox outbreak in Yugoslavia to the public health response, which included contact tracing, quarantines, lockdowns, and mass vaccination. Was that indeed the case?
The Course of the Outbreak
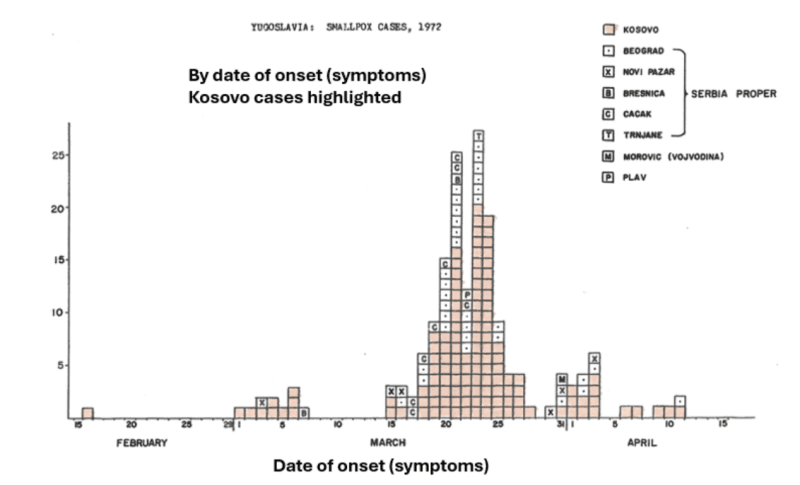
The epidemic graph (below) was taken from the WHO document. I added the blue curve. The index case, a villager from Kosovo, was identified in February and was probably infected during a trip to Mecca. Reportedly, he was vaccinated in his youth and received the obligatory vaccine against smallpox before his trip “without a control of vaccination success.”
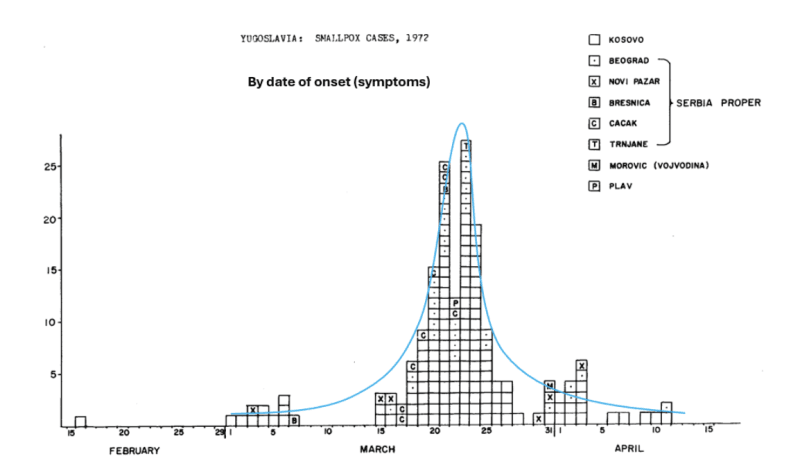
The WHO document refers to “three generations” of the outbreak based on presumed chains of infection, or what they imagined as three waves: two small and one large in between. In fact, we observe a classical, single epidemic curve that peaked on March 23. (Allowing for some randomness in the date of a few cases should eliminate any doubt about the underlying bell-shaped distribution.)
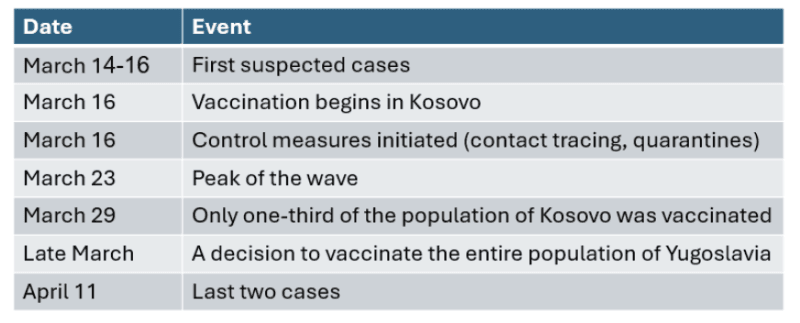
The timeline of the outbreak and the public health response are summarized in the table. It was about four weeks between the detection of the first cases and the last cases.
Of 175 cases, 124 (71%) were Kosovo residents. They are highlighted in the graph below. The wave pattern is evident both within and outside Kosovo.
The incubation period of smallpox was at least one week long and might have been as long as two weeks. Here is what the WHO document states on the topic, based on the presumed date of contact with an infected person.
“For 88% of the patients, the incubation period ranged from 9 to 13 days. These observations are in accord with those described in the literature.” Shifting the graph of cases (displayed by date of symptom onset) to the left by 9 days, we get an approximate graph by date of infection. The arrows indicate three milestones.
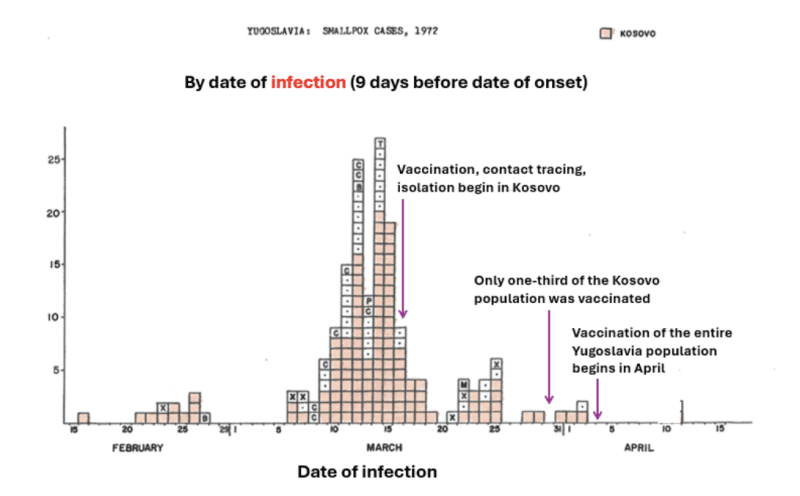
The graph shows that the number of infections peaked and declined before any public health intervention.
Note that a shift of the symptom-based graph by 9 days is conservative. The mean incubation period in the outbreak was 11 days, placing March 16—the date of the first interventions—well within the tail of the infection-based wave. Moreover, no intervention has an instantaneous effect on the risk of infection.
In summary, it was a self-limited epidemic wave, mainly concentrated in the Kosovo population whose unique characteristics will be described later. Most likely, the panic-triggered official response added close to nothing and caused collateral damage.
The Public Health Response
A series of quotes from various publications should give an idea of the measures that were taken in Yugoslavia:
“On 16th March, when virological examination confirmed the diagnosis of smallpox, martial law was declared.”
“Measures included blockage of villages and neighborhoods, roadblocks, prohibition of public meetings, closure of borders, and prohibition of non-essential travel.”
“The main form of isolating contacts in Kosovo was to place villages under quarantine, during which no one was allowed to leave or enter without special permission.”
“All wards and beds of Djakovica Town Hospital were placed at the service of the battle against the smallpox epidemic. Treatment of other medical conditions was practically suspended.”
“During the epidemic, the Kosovo police intervened 718 times for violation of the ban on gathering, 166 times for tracing contacts, and forcefully took 14 potentially infected persons to quarantine. The police also oversaw the process of vaccination.”
“Vaccination of the population in the first hotspots in Kosovo began on 16th March and was subsequently expanded in concentric circles…”
“By 29 March a total of 400,000 people, or one-third of the population of Kosovo, were vaccinated.”
“The freedom to choose not to be vaccinated did not exist in Yugoslavia in 1972.”
“On 24 March the Yugoslav government held an extraordinary meeting to discuss the smallpox epidemic. Citizens were called on not to leave their places of residence unless absolutely necessary…”
“On 26 March, Bulgaria sealed its border with Yugoslavia, and Hungary restricted entry to Yugoslavs who had a vaccination certificate.”
“In late March the Yugoslav Epidemiological Commission decided that the entire Yugoslav population, or 18 million people, should be vaccinated.”
Sound familiar?
On the Limited Nature of the Outbreak
To understand why the epidemic ended without external interventions, we should revisit the concept of herd immunity.
Smallpox ceased to be a public health threat in the last century in part because the quality of life improved in many places. Living conditions, sanitation, hygiene, and nutrition in the 20th century were drastically better than before. The smallpox virus needed a highly vulnerable host, not merely a host, and the condition of the population it encountered had changed. Apparently, the herd immunity level at which an epidemic is prevented or peaked is a broader concept than is narrowly defined. It is not just immunity from previous infection or vaccination. Neither played a significant role at the outbreak.
The population of Yugoslavia was far from being protected by previous smallpox vaccination, if at all. The most optimistic estimates of coverage were well below 50%. Moreover, we’ll see later that previous vaccination in childhood was not associated with a reduced risk of infection in the adult population. Likewise, the last case of smallpox was reported 40 years earlier.
The wave peaked quickly because a high level of herd immunity has been present—without prior infection or protection by vaccination. However, it was lower in Kosovo.
The ethnic composition and the socio-economic status in the Province of Kosovo (a population of 1.1 million) markedly differed from other locations in Yugoslavia. The majority were ethnically Albanian and predominantly Muslim. Many people were still living in poor conditions, as reflected, for example, in a higher incidence of infectious and digestive diseases than elsewhere in Yugoslavia. Likewise, the infant mortality rate was still high compared to the rest of Yugoslavia.
Here are descriptions of the social conditions, taken from several sources:
“Kosovo was the poorest and least developed region in Yugoslavia…In addition to chronically low access to clean water and a lack of adequate sewage systems came a heavy population density and a high rate of unemployment.”
“The population was composed of large extended families…The average number of household members in Kosovo was far higher than in other parts of Yugoslavia…There was the custom that everyone ate and drank from the same dish and slept together in the same bed.”
“The Albanian families in Kosovo in which someone fell ill with variola [smallpox] were usually poor and lived in poor housing conditions. The parents in those families usually had more than four children, and all household members shared the same eating and drinking vessels and the same sleeping space…The doctors sent to Djakovica during the epidemic observed quite a low level of health and hygiene awareness in the general population.”
A clear picture emerges from these quotes. It was a population whose standard of living resembled the 19th century in some respects.
Still, even in Kosovo, the level of herd immunity—in its broader sense—was sufficient to terminate the outbreak so quickly. Neither previous infections (< 100) nor previous vaccination (low rate, short-term protection, if any) nor public health interventions (late) could have explained why the wave peaked within a few weeks at about 20 infections per day. In other locations, the wave peaked at about the same time with only a few infections per day. Therefore, new outbreaks were unlikely to happen. And if they did, they would likely have been similarly small. Smallpox was not a public health threat in Yugoslavia in 1972. It was a public scare.
The Smallpox Vaccine
A question of obvious relevance is the effectiveness of the smallpox vaccine. The authors of the WHO document presented the following data about the vaccination status of the cases (transcribed from the original table).
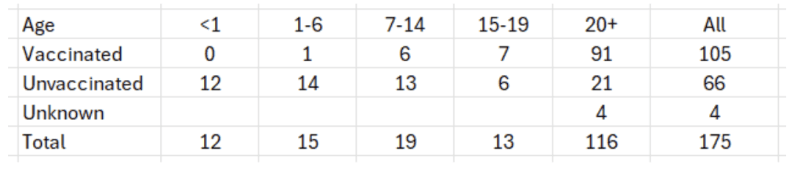
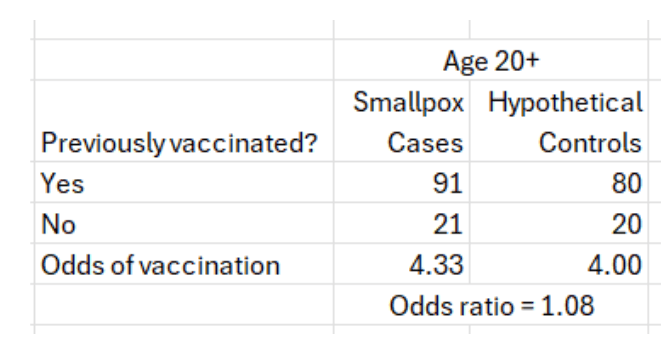
Reading the report, there is little doubt that the authors connect the infection to non-vaccination. This, however, is a case-only study. There are no controls. To estimate the odds ratio, a measure of association between vaccination status and infection status, we need the same kind of data on controls, or simply data from the respective population. For instance, the odds of having been vaccinated in cases age 20+ were 91:21. What were the odds of having been vaccinated in that age group? If previous vaccination was effective, the latter odds should have been higher (odds ratio < 1).
The vaccination status of the population of Yugoslavia was uncertain, but even the most optimistic estimate is no more than 80% of adults. For example:
“In some areas, the coverage of the population with smallpox vaccination was significantly lower than the legally recommended minimum of 80%, with significant variations in coverage between certain parts of Yugoslavia. Estimates indicated that 25% of the population was vaccinated…”
One source explains the circumstances:
“Smallpox was eradicated in Yugoslavia in 1930, sooner than in the United States. After that, Yugoslav children were vaccinated against the virus at 18 months, at 7 years and at 14 years. Part of the male population was vaccinated during military service, which was compulsory for men aged between 18 and 27. Medical personnel were supposed to be vaccinated frequently, which wasn’t always the case. Other failures of the health care system also came to light, including resistance to vaccination measures, and claims that false vaccination cards and exemption certificates were in circulation.”
Naively assuming 80% coverage, the odds of having been vaccinated in the adult population were about the same as the odds in adult cases. There is no evidence of any residual effectiveness at the time of the outbreak.
At any rate, it was assumed that revaccination would be effective in the short term. How effective was previous vaccination in young children, an indicator of short-term protection at the time of the outbreak?
Based on their “case-only” data, the authors of the WHO document thought that it must have been effective. They wrote:
“All cases among those less than one year of age were among the unvaccinated [12 infants]. In the age-group 1-6, the age-group in which most children should be protected by primary vaccination, only one of the 15 patients had been vaccinated.”
None of the sources tell us how many were from Kosovo, but we find the following sentence:
“In Kosovo, 30 patients were aged 1-7 years, whereas outside Kosovo only one patient was under 8 years of age.”
If so, all infants (<1 year) were from Kosovo, and at least 14 children (out of 15) between ages 1 and 6 were from Kosovo. We may therefore conclude that hypothetical controls should originate from Kosovo. What were the odds of having been vaccinated in Kosovo up to 6 years of age?
As was mentioned earlier, the population of Kosovo was predominantly Muslim, and they often refused to be vaccinated for religious reasons. Adding the lack of knowledge (or care) about basic hygiene and a remote disease they had never encountered, it is likely that the odds of finding a vaccinated infant or child among hypothetical controls from Kosovo were about zero.
In short, the implication that non-vaccination has contributed to the risk of infection in this age range cannot be inferred from the data. It is equivalent to inferring that smoking [non-vaccination] has accounted for lung cancer [smallpox] from a study of a population where everyone smokes [everyone is unvaccinated].
We have already seen the ineffectiveness of a previous vaccination in the adult population of Yugoslavia. In the remaining age groups, a substantial proportion of the cases have been vaccinated, implying that an unknown proportion did not live in Kosovo. Here, we have inherent confounding: non-vaccination was associated with living in Kosovo, where the risk of infection was higher to begin with. It is impossible to offer any theoretical computation.
I am wondering why epidemiologists at the WHO or in Yugoslavia failed to obtain the crucial vaccination data on controls from each age group. The case-control design was relatively new in the 1970s, but epidemiologists were familiar with the famous case-control studies of smoking and lung cancer two decades earlier. Either they were confident about the effectiveness of the smallpox vaccine, or they suspected that the computation might produce disturbing results.
In summary, the vaccination data indicate the ineffectiveness of vaccination years before the outbreak and cannot be used to infer even short-term effectiveness.
Adverse effects?
One source tells us that “The available reports do not specify the frequency of adverse reactions following vaccination.” But they add, “Among the vaccinated, there were many pregnant women who were vaccinated within the first 3 months of pregnancy, and most of them had an abortion [citing a reference is Serbo-Croatian].”
Hospitals
Hospitals are for the sick, but as every physician knows, hospitals are also a dangerous place: medical errors, unnecessary procedures, and nosocomial infections—to name common risks. The WHO document includes a table that shows the number of infections that occurred in a hospital setting in various locations.
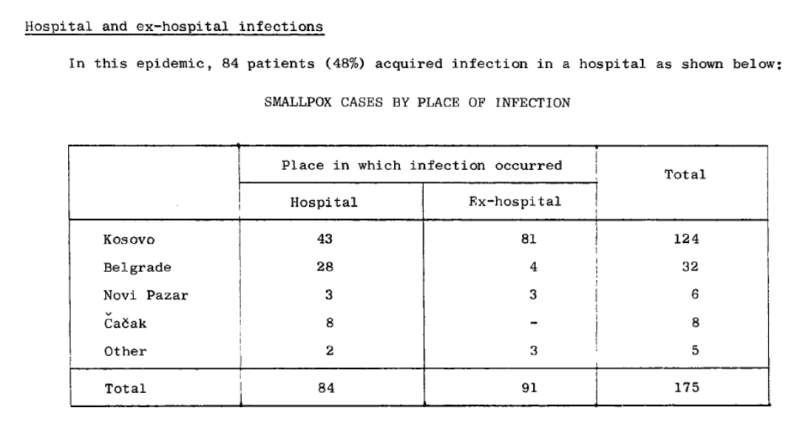
Most infections outside Kosovo (80%) happened in the hospital. Indeed, hospitals are a high-risk environment during an epidemic—for patients, visitors, and staff.
A proper ending for this piece may be a few summary statements from various sources (italics added).
“The effective management of Yugoslavia’s smallpox epidemic has drawn much interest from contemporary observers of the current COVID-19 pandemic.”
“The epidemic, which caused 175 cases and 35 deaths, was brought under control 6 weeks after the first diagnosis of smallpox.”
“The outbreak was brought under control using mass vaccination.”
“It also illustrates very well how even the most alarming outbreak can be brought rapidly under control by an efficient public health organization…”
Apparently, some minds cannot accept the idea that epidemic waves end naturally, and no amount of data can bring those minds under control.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








