
If there is one thing we have learned since 2020 it is the power of confirmation bias. The public health establishment has presented a mass of data and analysis to show that it was right all along about the Covid-19 pandemic and saved millions of lives. This finding has been accepted at face value and incorporated into policy, but rests on shaky foundations.
We need to look at the big picture. Apologists for vaccination generally use point-to-point comparisons – they pick an arbitrary date near the peak of the epidemic curve and compare it to a later date to show that an intervention is correlated with a reduction in infections or mortality. This is open to case-counting window bias and immortal time bias – another selection of dates could yield an entirely different result.
To counteract this, we need to look at the epidemic curve as a whole and see whether the intervention changed its trajectory.
What we see in the Euromomo statistics of European all-cause mortality below, is a series of declining peaks and broadening curves after the anomalous peak in April 2020. All-cause mortality is crucial, as it avoids distortion due to misclassification of deaths between Covid-19, vaccine adverse effects, and other causes of death.
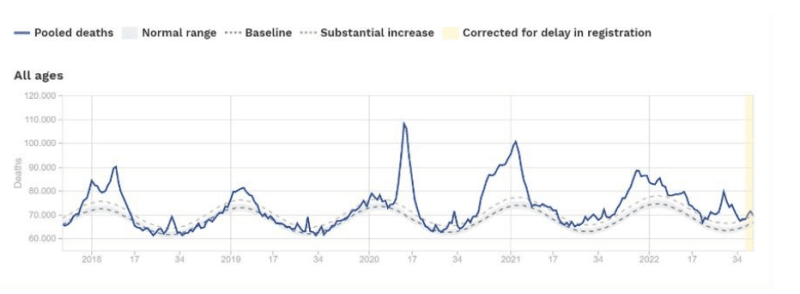
There was a gradual return to a more normal pattern, usually attributed to a combination of increasing natural immunity and the effects of vaccination. This falls far short of the exaggerated claims made for vaccination when the first clinical trial results were released. We were told by political and public health leaders that vaccination gave 95% protection, a figure that was based on the rate of Covid-19 symptoms paired with positive PCR tests in the vaccine group, compared with the placebo group. It was not based on improved mortality.
Vaccination may have contributed to the improving trend, but there is no basis for finding that it was solely responsible for returning to a more normal seasonal pattern of mortality. And hidden in the count of all-cause excess mortality may be deaths caused by Covid-19 vaccination. There is no way of excluding this possibility.
For example, vaccine-related deaths could be driven through cardiac adverse events. The Cohort study of cardiovascular safety of different Covid-19 vaccination doses among 46 million adults in England by Ip et al showed that incidence rates of cardiovascular events were substantially higher (nearly double for arterial events) after the first dose of the Pfizer and AstraZeneca vaccines, compared to no vaccination (Table 2).
The authors then concluded the opposite by adjusting the figures. But they selectively only employ adjustment factors that place downward pressure on vaccine hazard ratios, and ignore factors that might exert upward pressure, such as the well-known healthy vaccinee bias.
Chemaitelly et al corrected for this by assessing the association between Covid-19 vaccination and non-Covid-19 mortality as a control. They found that ‘A pronounced healthy vaccinee effect was observed during the first 6 months following vaccination, despite meticulous cohort matching,’ possibly due to seriously ill individuals not being suitable candidates for vaccination and so being underrepresented in the vaccinated group.
Some studies adjust for case-counting window bias or immortal time bias, but healthy vaccinee bias is too problematic to correct, so the full range of confounding effects is not brought to bear on the results, leaving the field to partially corrected studies which may be more misleading than uncorrected results.
Finding our way through this maze is difficult and the mass of observational studies are not a reliable basis for public health policy.
Have pandemics ever been defeated by vaccination? The greatest case study of them all is said to be polio vaccination. Everyone knows that the world was saved from polio by vaccination – and yet in fact it made no difference to the trajectory of polio cases in the 20th century.
Here is a graph showing the incidence of polio cases in the US over the full course of the 20th century, compiled by Gemini:
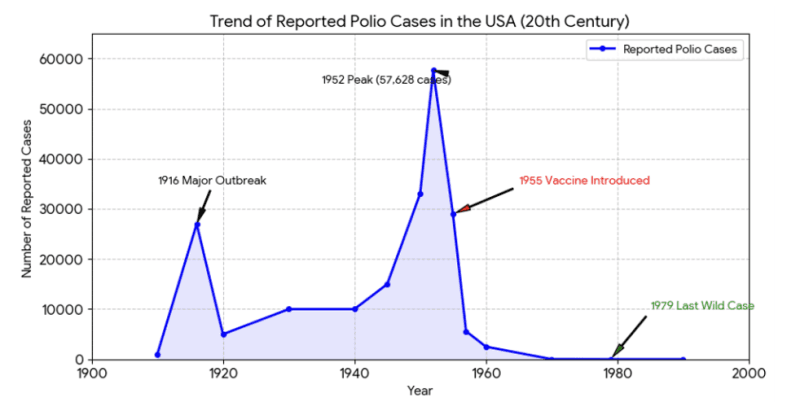
Over this period, there were two major outbreaks that built up rapidly to a peak and then quickly declined. The first was entirely prior to vaccination and vaccination was introduced towards the end of the second. The profile of both outbreaks is the same, and the trajectory of decline in the second one is almost unaffected by vaccination.
Notice that there were virtually no cases of polio before 1910, yet the absence of cases at the end of the century is attributed entirely to vaccination.
When vaccination is defended in the media, we are invariably told that polio was a horrid disease and we cannot go back to the days before vaccination when children had to be kept alive in iron lungs etc. But the 1800s were ‘before vaccination’ and polio was rare.
The big picture is that cases went from zero to zero over the course of the 20th century. There is no reason to believe that vaccination was responsible for the disappearance of polio after 1980, which was a reversion to the status at the beginning of the century, which clearly cannot be attributed to vaccination.
Measles is the other case study that is supposed to demonstrate the ability of vaccination to prevent epidemics and bring about elimination of a disease in a population. All media reports on measles outbreaks conclude that they are caused by downturns in vaccination and only vaccination can prevent them.
But the following graph of 20th-century measles cases provided by Gemini looks very similar to the polio graph, with peaks in the middle of the century and lows at the beginning and the end. Standardised reporting of measles began only in 1912, so the beginning of the rising trend that peaked in 1920 is unknown.
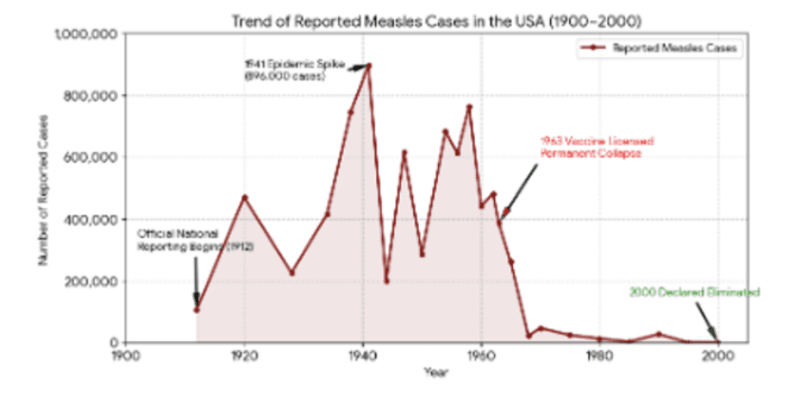
Proponents claim that vaccination is responsible for the prolonged (‘permanent’) low at the end of the century. But Gemini tells us that improved indoor ventilation, building design, and less crowded housing are also factors. It maintains these are less important than vaccination, without providing evidence for this.
Perplexity provided me with a summary of clinical studies showing the effectiveness of vaccination, including a large Cochrane study of the combined MMR vaccine leading to an estimate of 95% effectiveness against measles (sound familiar?). However, the Cochrane authors acknowledge:
Most of the studies included in this review were observational studies, therefore quantitative synthesis is performed on adjusted estimates by multivariate models.
In fact, all the studies summarized in Table 1 showing effectiveness against measles are observational studies, which aligns with the critiques made by vaccine sceptics that the evidence for vaccination is not based on the ‘gold standard’ of randomized controlled trials (RCTs), and is heavily adjusted. As we have seen above, adjustments can be made selectively for the ones that are favourable to the intervention only.
I asked Perplexity to designate which of its sources were RCTs. It produced one true RCT of the MMR vaccine by Zimakoff et al, which arrived at negative findings:
Findings of this trial conducted in Denmark, a high income setting, do not support the hypothesis that live attenuated MMR vaccine administered early to infants aged 5-7 months decreases the rate of hospitalisations for non-targeted infection before age12 months.
Medical science excels at the micro level. But we need to focus on the macro level to understand epidemics.
Health authorities are adamant that universal vaccination is essential to prevent epidemics of diseases such as Covid-19, polio, and measles. This is not supported by examining the trajectory of epidemic curves or by randomized controlled trials. The critics are right.
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








