
Academic communities have played a leading role in developing the response to the COVID-19 pandemic, and it is reasonable to assess their contribution. How did they exercise thought leadership, and how constructive was it? How did they influence the national decision-making processes and how did they make their own decisions?
The conventional narrative will maintain that experts have been crucial in identifying the threat in the first place and then devising effective strategies to counteract it.
These same experts magnified the threat from the novel virus and used it to justify novel strategies without due deliberation on the costs and benefits. The established strategies in previous pandemics focussed on quarantining and treating the sick, but these were abandoned in favour of universal strategies targeting the whole population in a way never before seen, when little or no evidence was available that they would be more successful than the established methods. This was a revolution in pandemic management policy, built on sand, so to speak.
The revolution was sparked off by perceptions that China’s authoritarian approach had successfully suppressed the virus, followed by dodgy modelling used to recommend a similar approach in the West. Modelling generates hypothetical scenarios, which are not evidence. Hypothetical scenarios should not be used to generate policies that create mass harms in actuality.
Imperial College London’s COVID-19 Response Team took the lead, recommending ‘suppression’ instead of ‘mitigation,’ although even their own results did not demonstrate that suppression would lead to superior outcomes. Policymakers were spooked by the predictions that there would be 510,000 deaths in the UK and 2.2 million in the US in the ‘do nothing’ or ‘unmitigated’ scenario. Since this scenario never eventuated these predictions are not falsifiable.
Modelling groups around the world took up the baton and reinforced the ICL team’s recommendation, in which universal restrictions on movement would be imposed for a period of eighteen months or so until an effective vaccine could be developed. A one-size-fits-all model took hold, in which everyone in the entire world (including healthy people) should be quarantined in their homes for the first time in history, followed by coercive policies designed to vaccinate every single individual in the world with untried, novel vaccines.
These were extreme and draconian policies, and it is important to review the governance model that was followed to make these decisions, first within the universities themselves. But the university decision-making processes can also be used as a microcosm for the way governments went about making their decisions. Similar decision-making processes were followed in universities, corporations, local and regional and national governments. And the same weaknesses in these processes are evident at each level.
In some past golden age, we like to think that university decision-making was characterised by collegial debate, in which a diverse range of options and arguments were canvassed, tested against the evidence, and then the best approach adopted. This golden age probably never existed, but it represents an ideal that we should not lose sight of. A university, of all places, should ensure that the full range of tenable perspectives and strategies is considered before a policy decision is made. And there should be a full consideration and evaluation of the strength of the evidence supporting each position. This concept of collegiality rests on the idea that the intellectual value of the opinions of each member of the university community can only be based on the strength of their arguments and the evidence underpinning them, not on their seniority in the organisational hierarchy.
In the case of pandemic policy, decisions should take full account of the scientific evidence on parameters such as the infectiousness of the virus, its transmissibility and the vectors of transmission, and the strength of the evidence that each of the available strategies might be effective. If the parameters are not yet known, this should lead policymakers to proceed with caution.
From early on in the pandemic, two schools of thought emerged, one represented by the John Snow Memorandum, which advocated universal methods, and the other by the Great Barrington Declaration, which advocated ‘focussed protection.’ There was almost no ongoing debate in the academic community about the relative merits of these two strategies, but rather a premature closure.
The John Snow Memorandum claimed to represent the ‘scientific consensus.’ This was self-evidently misleading as a consensus exists when there is general agreement, whereas the whole purpose of the John Snow Memorandum was to oppose the supposedly erroneous ideas of the Great Barrington Declaration. This was despite the fact that the Great Barrington Declaration was based on the actual scientific consensus that was in place until 2020, which was hastily abandoned within weeks without rigorous exploration of the evidence.
The pro-lockdown group managed to persuade the media and governments that they did indeed represent the consensus scientific view and this was accepted by the universities themselves, and then by governments, without any attempt at critical probing of its merits, a necessary condition of good governance. Once sufficient data accumulated to make some assessments of the success of lockdown strategies, diverse findings emerged in the literature, with favourable assessments largely based on modelling, whereas more empirical assessments were less favourable. According to the Johns Hopkins Meta Analysis by Herby et al, reliable empirical studies showed that mortality was reduced in the first wave by somewhere in the range between 0.2% and 2.9%, depending on the methodology used. This modest short-term gain needs to be offset by the medium-term increases in excess mortality that are becoming evident in 2022, not to mention severe mental health crises, especially in young people in both cases.
Universities fell in with the prevailing conventional strategy which tried to prevent the spread of the virus, firstly by closing campuses down, and then by making it compulsory to be vaccinated in order to come back onto campus. Each university tried to make the campus an infection-free zone, each university leader tried to be King Canute, forbidding the virus to pass the ‘cordon sanitaire’ around the walls.
How did that go?
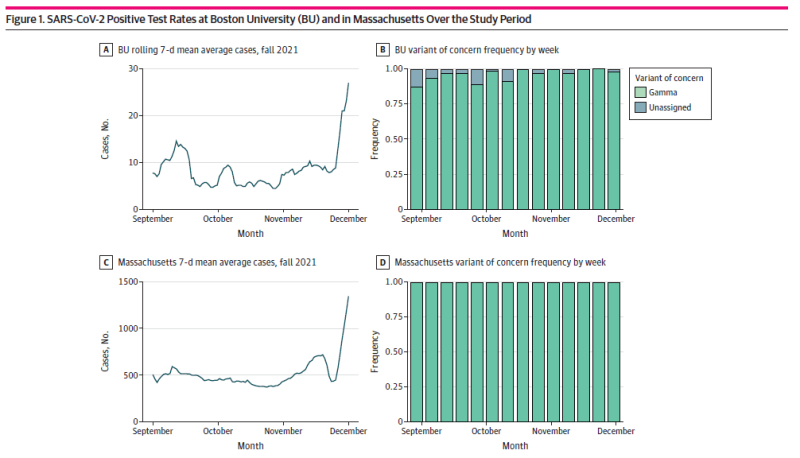
There have been a number of papers specifically exploring the outcomes of university campus control measures including lockouts (of the unvaccinated). One team undertook a cohort study (using contact tracing and polymerase chain reaction analysis) over one semester in 2021 at a Boston University campus during a period when on-campus classes had resumed, but there was compulsory vaccination and use of face masks. The results indicated that there were few on-campus transmissions but there was no control group, so it is difficult to conclude that this was caused by the policies, as opposed to confounding factors. And Figure 1 in this paper clearly shows that cases on campus went through the roof at the end of 2021 in sync with cases in the surrounding community, so it is hard to see that overall outcomes were in any way improved. Shutting the campus down again would not have helped as students were being infected predominantly in the general community.
A similar study was undertaken at Cornell University over the same period. The starting point was:
Vaccination was mandated for all students and encouraged for employees. Masks were required on-campus, and isolation orders and contact tracing occurred within hours of any positive result. We hypothesized that these measures would limit COVID-19 spread on campus and sought to monitor this with a case-series study of university testing records.
Whereas, in fact, the hypothesis was falsified:
Cornell’s experience shows that traditional public health interventions were not a match for Omicron. While vaccination protected against severe illness, it was not sufficient to prevent rapid spread, even when combined with other public health measures including widespread surveillance testing.
Despite the predictable claim that vaccination protected university community members against severe illness, neither study in fact measured this outcome.
The total outcomes at both Boston U and Cornell show the futility of attempting to erect a wall around any territory to prevent waves of infections from coming in through border controls (unless perhaps you are an island). Neither university was able to ‘stop the spread’ or ‘flatten the curve.’ Similar conclusions were reached by a study of three of the universities in Massachusetts and New England. The complete failure of the control measures should have led to their reassessment and removal.
The original decision to lock down, and even more the decision to exclude the unvaccinated from the universities, should have been made after a vigorous debate in the academic senate, with both pro and contra arguments given full rein. Did this happen anywhere?
Unlikely – the modern university is not run by the academic staff anymore, not even by the professors. As universities became larger and more difficult to manage with budgets in the billions of dollars and students in tens of thousands, and even more than 100,000, power transitioned to the managerial class, leading to a prevailing ethos of ‘managerialism.’ University governing bodies are characteristically made up of majorities of external members, many of whom have little understanding of the obscure arts of academic quality assurance and effective teaching and learning. Therefore, they leave these matters to be handled by the Academic Senate and the university managers.
The managers and the governing body are increasingly preoccupied with the efficient allocation of resources and the organisation of the university within ever-changing bureaucratic structures. Academic staff carry out their functions within bureaucratic organisational units and are subject to ‘performance management’ which favours reliable performance within conventional forms, and conformity with norms over erratic brilliance. Remember that Einstein wrote four of his most groundbreaking papers in his spare time before he was able to gain a university position. So, the bureaucratic university becomes a ‘factory of learning.’ focussed on achieving utilitarian vocational outcomes for students – higher training, not higher education.
When a decision comes before the governing body such as a proposal to shut the university campus down or to force all staff and students to be vaccinated on pain of banishment, the decision-making process will take a bureaucratic form, not a collegial form. Management will put together a brief and a recommendation. The brief will not contain a comprehensive overview of the different findings in the science. If ‘the science’ is mentioned at all, the brief will present the fake consensus and present the science as monolithic and uniform or ‘reified’ (a term much loved by academics). Unconventional or contrarian perspectives will not be included. Management will maintain that the measures have to be undertaken in order to preserve a safe working environment.
However, the risk of mortality from COVID-19 rises exponentially with age and university communities have a relatively young age profile, so the risk on campus was always markedly lower than in, for example, aged care homes. And the ability of the vaccines to prevent transmission was always weak and short-term, and probably non-existent in the age of Omicron dominance. It was never clear that the benefits would exceed the risks or that the policy objective would be achieved, but every governing body duly voted for management’s recommendation. This is because governing bodies will always follow the conventional path.
If the local health authorities recommend something, no university president or governing body member will oppose it, and none will undertake an independent assessment. They will take a fundamentally defensive approach – the priority is to avoid being criticised for not taking the recommended action, even if the action proves to be futile or counterproductive. Because they are essentially symbolic, they are not easily subject to being revised in the light of actual experience.
This organisational decision-making model is replicated at the higher levels of government. The safest course for governments is to accept the ‘health advice’ given to them by the various agencies and advisory committees of Sages. This health advice will inevitably present the fake consensus and governments will not be told that alternative strategies exist that need to be considered. Any references to ‘the Science’ will be filtered to ensure that decision-makers don’t get to know about diverse findings and unconventional viewpoints are not presented or presented minimally framed by dismissive comments. The conventional or established view will be presented as the consensus view, and these have been consistently confused throughout the pandemic.
The outcomes for nations over the northern winter of 2021-2 was the same as for the universities. Trying to control national borders was no more successful than trying to control campus borders. Curves were not flattened, which can be seen immediately in the graphical evidence.
Both universities and governments imposed extreme policies, extending to the micro-management of everyday life during lockdowns and gross violations of human rights, including the right to bodily autonomy. These extreme policies were not supported by hard evidence of effectiveness either at the time or since.
Vocal academic experts repeatedly took the lead in calling for these extreme policies, backed by the authority of science. But their policy recommendations were based on opinion, not on consistent scientific findings, and the full range of academic viewpoints and findings was not considered. This was a new kind of ‘trahison des clercs,’ with dire consequences that are starting to emerge.
What can be done to avoid similar mistakes being made in the future? There are profound implications for how courses are taught in our universities, especially the vocationally-oriented ones. They need to be opened up to more viewpoint diversity. They need to develop strategic thinking in their students (and staff!), not just technical skills. The prime objective of any professor must be to develop the student’s capacity for independent evidence-based thinking and critical inquiry.
Medical schools need to be more open to integrative medicine as opposed to just pharmaceutical medicine. The editor of the Lancet, the voice of the British medical establishment, published an opinion piece in September 2020 with the provocative title ‘COVID-19 is not a pandemic.’ He characterised it rather as a ‘syndemic,’ because ‘addressing COVID-19 means addressing hypertension, obesity, diabetes, cardiovascular and chronic respiratory diseases, and cancer.’ Almost all the people who have died had one or more of these conditions.
When devising strategies to solve any problem it is critical to first characterise the problem accurately – the virus was the trigger, not the sole cause. This important contribution was completely ignored and the narrow focus on the war against SARS-Co-V2, the virus, continued. Governments made no attempt to address the so-called ‘comorbidities.’ The WHO’s so-called ‘integrated’ Strategic preparedness, readiness and response plan to end the global COVID-19 emergency in 2022 completely ignores them and focuses only on the narrow biosecurity agenda.
The decision-making processes of organisations, agencies and governments need to be opened up, especially when these fateful policy decisions are being made that affect the lives of the community with such impact. There has been too much premature closure. There must be sufficient divergent, exploratory thinking before entering the convergent phase leading to decision. Collegial discussion and debate need to return to universities when these sorts of decisions are being contemplated, and genuine parliamentary debate in the case of governments. And the briefs given to governing bodies must be structured in such a way that they systematically contain consideration of all tenable positions and all the available evidence.
This will not happen by itself, and so the bureaucratic framework needs to be changed to work against its innate tendencies towards conformity. Policy makers should write their briefs in accordance with protocols that require respectable contrary viewpoints to be given due weight. The policy framework must support continuous improvement instead of reinforcing the status quo. And there must be a genuine cycle of review of the outcomes of major policy decisions, one that is capable of changing directions when policies fail to achieve their objectives.
The first step in this process is to define the objectives clearly at the outset, so that progress can be measured. Throughout the pandemic, government objectives have been referred to in ad hoc remarks in press conferences and have been ever-changing, which makes it possible to fudge any outcome as being in some way achieved.
In other words, the bureaucratic model of decision-making must support a rigorous dialectical or collegial model of due deliberation, both in universities and in governments. And this dialectical model needs to become systematic and entrenched.
Open universities should support open government and the open society.
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








