
The 2021 US Open is beginning this week and Novak Djokovic is going for both a Grand Slam (first men’s in over fifty years) and the all-time lead in Grand Slam men’s singles titles wins. Suppose Djokovic decided to bet $2.5 million on himself, the winner’s purse. It’s against the rules, but hypothetically, before the tournament begins, is there a greater endorsement of what you believe in than putting your own assets on the table?
Pete Rose did that, betting on his Cincinnati Reds to win games. Yes, it violated MLB rules, he had access to his and his opposing team’s health and motivation, and yes, it was unethical. Still, betting on yourself is the ultimate display of confidence.
COVID-19 vaccines have been out for nine months. The two mRNA vaccines are manufactured by Moderna and Pfizer, and the DNA-based vaccine by Janssen (Johnson and Johnson). The mRNA’s were represented early on to present a 95% efficacy in preventing serious illness, hospitalization or death. The Janssen vaccine is more traditional in its technology, modifying an adenovirus DNA with some of the SARS-CoV-2 virus to produce an immunity response. The J&J vaccine was represented to produce a 66% efficacy against moderate to severe COVID-19 and 100% against death.
As of September 1, 2021, we are seeing decreased efficacy for at least the mRNA vaccines. It’s clear they do not prevent COVID-19 infection; there are countless breakthrough infections. It’s also clear based on data from Israel, the UK and even in the U.S. where it’s reported that there are people getting sick and dying from COVID-19 that are vaccinated (many fewer than unvaccinated at this date).
The vaccines don’t have a 95% efficacy against serious illness, but it’s not zero either. This is not an anti-vaccine argument; I took the Janssen shot in May 2021. I’m not in an at-risk class; I’m thin and fit with no underlying conditions. I’m also over fifty, so there may be some breakeven point on my profile of getting vaccinated versus getting COVID-19. Most of my friends have gotten COVID-19. The only one that got sick (and hospitalized) is pushing sixty and overweight. I lost one family member to COVID-19 in a care facility in Michigan in April 2020.
COVID-19 Activity in Highly Vaccinated Communities
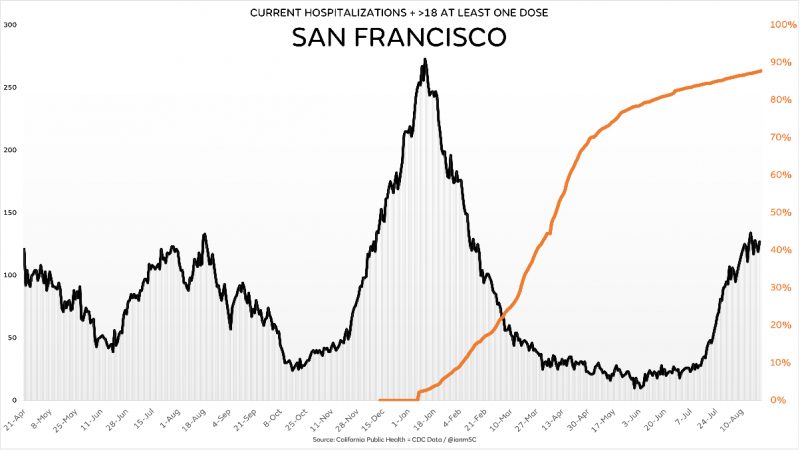
If vaccine mandates were a logical requirement, the vaccines should have irrefutable data support that they suppress infections, spread, the need to wear face masks (mandates are back in many places for the vaccinated) – in short to do what other vaccines have accomplished. Below is a chart (provided by @ianmsc) showing San Francisco’s trend of those vaccinated and COVID-19 hospitalizations. San Francisco is one of the most compliant large communities in the U.S., following guidelines like wearing masks, getting vaccinated, social distancing and other mitigations when they were required or recommended. While doing so, they are at the same number of raw COVID-19 hospitalizations they were at a year ago, that with close to 90% of the over-eighteen population vaccinated.
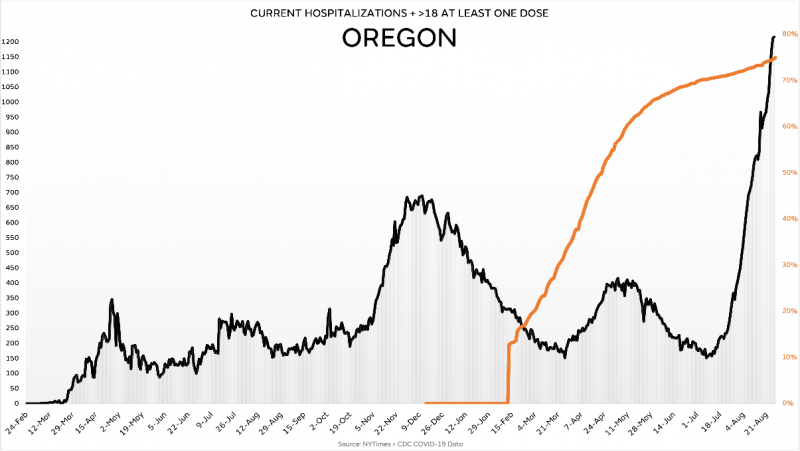
Oregon was largely spared significant COVID-19 hospitalizations and deaths throughout the first year of the pandemic. While they implemented stricter measures and kept more kids out of school than any state other than Hawaii, Washington, and California, they also had one of the lowest COVID-19 and excess death tallies in the country (Washington and Hawaii were also low in those categories; California was a leader in all-cause excess deaths). Still, four months after vaccinations reached over two-thirds of their over-eighteen population, they have far more COVID-19 hospitalizations than ever.
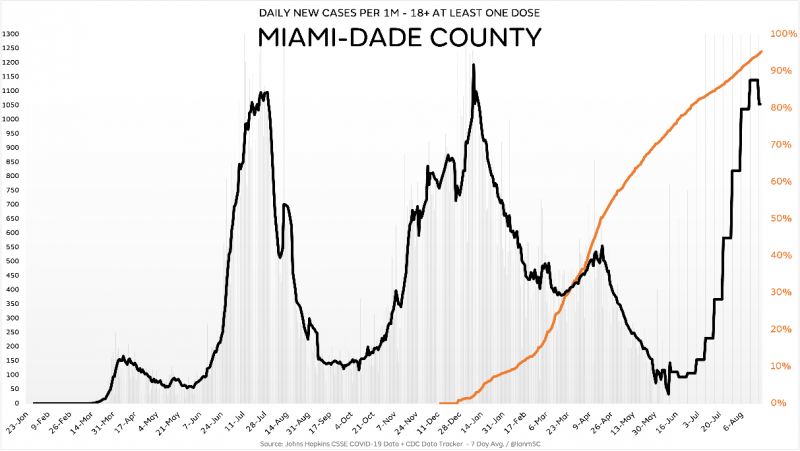
Florida has been the focus of much media attention this summer for the rise in COVID-19 activity. Miami is the most densely populated community in Florida, and many people are driven indoors in the summer because of the heat, like most of the southern states. With a ridiculously high vaccination rate in those over eighteen, they have seen cases comparable to a year ago. Hospitalizations were ~20% lower than a year ago, which may illustrate a combination of vaccine and recovered infection immunity at play.
Cases in highly-vaccinated Israel are at an all-time pandemic high. Israel is now requiring third Pfizer shots to qualify as “fully vaccinated.” There is no long-term trial or study data supporting such an approach is safe or will be effective. It seems like the mRNA shots are more like an annual flu shot, where the hit rate is maybe 50% of matching the strain and less at preventing infection. I got the flu shot from 2016-2019 and got the flu each year, probably because I was traveling about a hundred nights a year in hotels.
Deaths are not following the case and hospitalization trends they did a year ago, or last winter. There is some decoupling, and a combination of recovered immunity, the vaccines and a Delta variant that is a little less lethal seems to be the difference. We can all probably agree that the vaccines are reducing the risk of COVID-19 in those at risk to some degree. The data does show that the vaccine efficacy is not what we understand a typical vaccine to be – practical insulation from infection and illness. Does that mean that everyone should be required to get the COVID-19 vaccines?
Smallpox was a very lethal disease that became a pandemic in the 1870s and resurfaced off and on for the next hundred years. At one time and in different places in the world, it accounted for up to a third of deaths in certain age brackets. It was highly infectious to young people and particularly deadly for those infected over 45 years old. There was no doubt this was a measurable and deadly disease for many age ranges, and to those with no underlying conditions.
The death rate for chicken pox (varicella) was about ten times higher for kids aged 1-14 and thirty times higher for kids ages 15-19 than COVID-19. When the vaccines were developed and deployed for both of these diseases, cases essentially vanished, and those diseases were “conquered.” The vaccines did stunt the reproduction, or spread, whereas we are not seeing similar suppressed reproduction post-vaccine for COVID-19.
COVID-19 Deaths
COVID-19 has officially claimed just over 4,000 lives in those under thirty years old. Based on CDC and data from the UK, in both countries the deaths in young people actually from COVID-19 were found to be fewer than half the official count as attributed to COVID-19. That rounds down to an infection fatality rate of about zero. Yes, there are outliers, but there are many things more lethal to young people than COVID-19, including the flu, getting in a car, a homicide or an overdose.
If getting vaccinated proved to prevent an infection spread to others including the vulnerable, you could make a case to get everyone vaccinated. The vaccines have proven to not stop infection nor spread, nor were they marketed to do such from the beginning if you followed the communications closely. With a very disproportionate age stratification of COVID-19 deaths, it begs the question why everyone must be vaccinated to function in society.
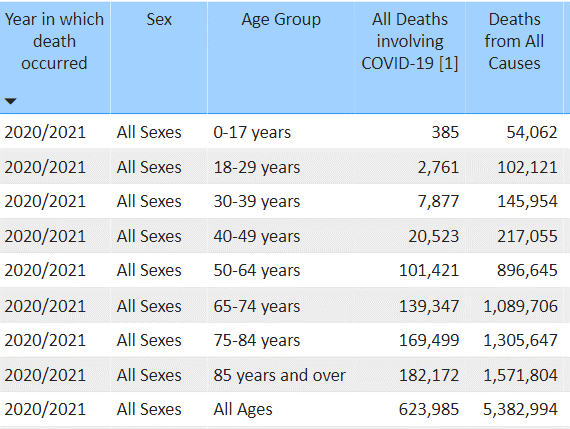
Source: CDC, through August 30, 2021
Vaccine Mandates
Many companies and education institutions are requiring vaccines for their employees and students. For employees to return to their offices to work, these companies are requiring employees to be vaccinated, now or in the future: Citigroup, Deloitte, Equinox, Facebook, Goldman Sachs, Google, Microsoft, Morgan Stanley, Netflix, the Washington Post and many others.
A friend works for a Fortune 500 manufacturing company in Dallas. His company is ready to announce a vaccine mandate for all employees. The CEO said in an internal townhall meeting last week that getting vaccinated was “smart, and if you don’t you’re willing to kill your co-worker’s children.” This is a CEO who is also on a board for another Fortune 500 company. They are implementing a vaccine mandate effective in October and if employees don’t get vaccinated, they will be terminated.
According to the Chronicle for Higher Education, 817 college campuses have vaccine mandates in place. These include hundreds of private schools, as well as large institutions like University of Michigan, Duke, Indiana University, Louisiana State University, MIT, most schools in California, Ohio State, Illinois and Michigan State.
A number of the schools requiring students be vaccinated are not requiring all employees to be vaccinated. It’s interesting in those cases that the lesser likely group to be affected by COVID-19 is required to be vaccinated, but the more likely group affected is not. Perhaps it’s because they can direct their customers better than their employees, an interesting inverse relationship.
I went to Michigan State University and follow what’s going on there often. Michigan State resides near the state capital, home to alumni Governor Gretchen Whitmer, who instituted a mask mandate for two-year-olds and up in March 2021, an order since rescinded when the state reduced her emergency powers. Vinay Prasad is also a graduate of Michigan State and is one of the more reasonable, outspoken, apolitical medical experts speaking out about the disproportionate responses governments and health experts have taken throughout the pandemic.
An employee of Michigan State University has filed a lawsuit against the university over the vaccine mandate. She got COVID-19 and has a test and antibodies to prove it. Still, she is being required to be vaccinated. There is no science or data to support the need for someone previously infected to be vaccinated. In fact, there are many studies and data points demonstrating that recovered immunity is many times more durable than vaccinated immunity, some of which is outlined here.
The question is – should vaccines be mandated for everyone when:
- They aren’t proving to stop the spread of SARS-CoV-2.
- They aren’t providing the symptomatic prevention as represented (though again, there is measured benefit to those at risk).
- The COVID-19 fatality risks for healthy young people are well over one in a million. The vaccines may have high efficacy for healthy young people, but being young and healthy yields about a 99.9986% success rate against severe illness or death without vaccination (that’s not an exaggeration). For context, if this were 95%, it would be catastrophic.
- The vaccines are having side effects in healthy people not at traditional risk of COVID-19. More healthy young people have likely gotten sick from the vaccines than from COVID-19, that data is loose on both sides but it’s possible (reference 1, 2 and 3). Teen male myocarditis is up 3,000% following COVID-19 vaccinations. No, the vaccines are not more dangerous than COVID-19 to the population at large, but they are causing more adverse reactions than any other vaccine in decades. They may well be riskier than getting COVID-19 for people not known to be at risk, particularly the young and healthy.
- Immunity following a SARS-CoV-2 infection is proving to be more durable than immunity following a vaccine.
If one believes in the vaccines, and they’ve been vaccinated, why are they concerned that a colleague, neighbor, child or teacher is not? One continued fail for the CDC and health experts has been highlighting exactly who is at high probable risk from COVID-19. Other than being over 65, being obese and having a severe COVID-19 reaction is most highly correlated. That message should be a part of every CDC COVID-19 update and emphasized in every news broadcast. It is not, and just in my circle, awareness of obesity risks has been very low.
Experts Know Their Business
Creators and designers and most employees know their company business better than anyone. Many people might know a bit about Tesla vehicles, but it’s highly unlikely any know more than the Tesla design engineers. Apple engineers understand their smartphone technology better than the people using it. Tiger Woods understands winning golf better than the people watching it on Sunday afternoons. The scientists at McCormick’s understand food flavoring at a different level that those consuming it.
Pfizer is not mandating their employees be vaccinated. This fall they will require weekly testing of any employees not vaccinated, at least that’s what it looks like now. Moderna is planning fall vaccine mandates for all employees, as is Janssen. Considering those vaccinated are able to get COVID-19 fairly regularly now (just in my circle, I know of over a dozen people vaccinated that have gotten COVID-19 in the last three weeks, in Texas), what is the endgame?
The vaccination rate in the elderly is very high in every state; it’s not necessarily in the obese. Some people I know working at two of the pharmaceutical companies (they are vaccinated or recovered from COVID-19) are skeptical the mandates will work, with those vaccine-producing company employees being experts on the COVID-19 risks and the risk/benefits of the vaccines.
The people at Pfizer, Moderna, Janssen and even frontline healthcare workers understand the science and data behind the vaccines better than anyone. If even a large minority of these people are reluctant or refuse to get vaccinated, it should tell us all something. COVID-19 is not a one-size-fits-all disease and should not be treated as such.
This brings us back to Novak Djokovic and the US Open. If Novak was able to bet on himself to win the US Open (assuming he is healthy), he’d probably put $100 million down on the championship, even if he gave it all away to charity. Will healthcare workers and employees at Pfizer, Moderna and Janssen bet on the vaccines? Let’s bookmark this column and see what healthcare workers and those that work at Moderna and Janssen do over the next six months.
It’s possible vaccine mandates for hospital workers, for teachers, for millions of corporate employees and the vaccine makers themselves will be curbed in this game of chicken.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








