If a plumber with a lifetime of experience were to tell you that water runs uphill, you would know he is lying and that the lie is not accidental. It is a lie with a purpose. If you can also demonstrate that the plumber knows in advance that the product he is promoting with that lie is snake oil, you have evidence for a deliberate con. And once you understand what’s really inside that bottle of snake oil, you will begin to understand the purpose of the con.
One of the most common reasons given for mass COVID vaccinations is the idea that if we reach herd immunity through vaccination, we can starve the virus out of existence and get our lives back. It’s the COVID-Zero strategy or some variant of it.
By now it is abundantly clear from the epidemiological data that the vaccinated are able to both catch and spread the disease. Clearly vaccination isn’t going to make this virus disappear. Only a mind that has lost its grasp on reality can fail to see how ridiculous all this has become.
But a tour through pre-COVID science demonstrates that, from day one, long before you and I had even heard of this virus, it was 100% inevitable and 100% predictable that these vaccines would never be capable of eradicating this coronavirus and would never lead to any kind of lasting herd immunity. Even worse, lockdowns and mass vaccination have created a dangerous set of circumstances that interferes with our immune system’s ability to protect us against other respiratory viruses. They also risk driving the evolution of this virus towards mutations that are more dangerous to both the vaccinated and the unvaccinated alike. Lockdowns, mass vaccinations, and mass booster shots were never capable of delivering on any of the promises that were made to the public.
And yet, vaccination has been successfully used to control measles and even to eradicate smallpox. So, why not COVID? Immunity is immunity, and a virus is a virus is a virus, right? Wrong! Reality is far more complicated… and more interesting.
This Deep Dive exposes why, from day one, the promise of COVID-Zero can only ever have been a deliberately dishonest shell game designed to prey on a lack of public understanding of how our immune systems work and on how most respiratory viruses differ from other viruses that we routinely vaccinate against. We have been sold a fantasy designed to rope us into a pharmaceutical dependency as a deceitful trade-off for access to our lives. Variant by variant. For as long as the public is willing to go along for the ride.
Exposing this story does not require incriminating emails or whistleblower testimony. The story tells itself by diving into the long-established science that every single virologist, immunologist, evolutionary biologist, vaccine developer, and public health official had access to long before COVID began. As is so often the case, the devil is hidden in the details. As this story unfolds it will become clear that the one-two punch of lockdowns and the promise of vaccines as an exit strategy began as a cynical marketing ploy to coerce us into a never-ending regimen of annual booster shots intentionally designed to replace the natural “antivirus security updates” against respiratory viruses that come from hugs and handshakes and from children laughing together at school. We are being played for fools.
This is not to say that there aren’t plenty of other opportunists taking advantage of this crisis to pursue other agendas and to tip society into a full-blown police state. One thing quickly morphs into another. But this essay demonstrates that never-ending boosters were the initial motive for this global social-engineering shell game ― the subscription-based business model, adapted for the pharmaceutical industry. “Immunity as a service”.
So, let’s dive into the fascinating world of immune systems, viruses, and vaccines, layer by layer, to dispel the myths and false expectations that have been created by deceitful public health officials, pharmaceutical lobbyists, and media manipulators. What emerges as the lies are peeled apart is both surprising and more than a little alarming.
“Once you eliminate the impossible, whatever remains, no matter how improbable, must be the truth.” – Sherlock Homes” ― Sir Arthur Conan Doyle
Viral Reservoirs: The Fantasy of Eradication
Eradication of a killer virus sounds like a noble goal. In some cases it is, such as in the case of the smallpox virus. By 1980 we stopped vaccinating against smallpox because, thanks to widespread immunization, we starved the virus of available hosts for so long that it died out. No-one will need to risk their life on the side effects of a smallpox vaccination ever again because the virus is gone. It is a public health success story. Polio will hopefully be next ― we’re getting close.
But smallpox is one of only two viruses (along with rinderpest) that have been eradicated thanks to vaccination. Very few diseases meet the necessary criteria. Eradication is hard and only appropriate for very specific families of viruses.
Smallpox made sense for eradication because it was a uniquely human virus ― there was no animal reservoir. By contrast, most respiratory viruses including SARS-CoV-2 (a.k.a. COVID) come from animal reservoirs: swine, birds, bats, etc. As long as there are bats in caves, birds in ponds, pigs in mud baths, and deer living in forests, respiratory viruses are only controllable through individual immunity, but it is not possible to eradicate them. There will always be a near-identical cousin brewing in the wings.
Even the current strain of COVID is already cheerfully jumping onwards across species boundaries. According to both National Geographic and Nature magazine, 40% of wild deer tested positive for COVID antibodies in a study conducted in Michigan, Illinois, New York, and Pennsylvania. It has also been documented in wild mink and has already made the species jump to other captive animals including dogs, cats, otters, leopards, tigers, and gorillas. A lot of viruses are not fussy. They happily adapt to new opportunities. Specialists, like smallpox, eventually go extinct. Generalists, like most respiratory viruses, never run out of hosts to keep the infection cycle going, forever.
As long as we share this planet with other animals, it is extremely deceitful to give anyone the impression that we can pursue any scorched earth policy that can put this genie back in the bottle. With an outbreak on this global scale, it was clear that we were always going to have to live with this virus. There are over 200 other endemic respiratory viruses that cause colds and flus, many of which circulate freely between humans and other animals. Now there are 201. They will be with us forever, whether we like it or not.
SARS: The Exception to the Rule?
This all sounds well and good, but the original SARS virus did disappear, with public health measures like contact tracing and strict quarantine measures taking the credit. However, SARS was the exception to the rule. When it made the species jump to humans, it was so poorly adapted to its new human hosts that it had terrible difficulty spreading. This very poor level of adaptation gave SARS a rather unique combination of properties:
- SARS was extremely difficult to catch (it was never very contagious)
- SARS made people extremely sick.
- SARS did not have pre-symptomatic spread.
These three conditions made the SARS outbreak easy to control through contact tracing and through the quarantine of symptomatic individuals. SARS therefore never reached the point where it circulated widely among asymptomatic community members.
By contrast, by January/February of 2020 it was clear from experiences in China, Italy, and the outbreak on the Diamond Princess cruise ship (more on that story later) that the unique combination of conditions that made SARS controllable were not going to be the case with COVID. COVID was quite contagious (its rapid spread showed that COVID was already well adapted to spreading easily among its new human hosts), most people would have mild or no symptoms from COVID (making containment impossible), and that it was spreading by aerosols produced by both symptomatic and pre-symptomatic people (making contact tracing a joke).
In other words, it was clear by January/February 2020 that this pandemic would follow the normal rules of a readily transmissible respiratory epidemic, which cannot be reined in the way SARS was. Thus, by January/February of 2020, giving the public the impression that the SARS experience could be replicated for COVID was a deliberate lie – this genie was never going back inside the bottle.
Fast Mutations: The Fantasy of Control through Herd Immunity
Once a reasonably contagious respiratory virus begins circulating widely in a community, herd immunity can never be maintained for very long. RNA respiratory viruses (such as influenza viruses, respiratory syncytial virus (RSV), rhinoviruses, and coronaviruses) all mutate extremely fast compared to viruses like smallpox, measles, or polio. Understanding the difference between something like measles and a virus like COVID is key to understanding the con that is being perpetrated by our health institutions. Bear with me here, I promise not to get too technical.
All viruses survive by creating copies of themselves. And there are always a lot of “imperfect copies” — mutations — produced by the copying process itself. Among RNA respiratory viruses these mutations stack up so quickly that there is rapid genetic drift, which continually produces new strains. Variants are normal. Variants are expected. Variants make it virtually impossible to build the impenetrable wall of long-lasting herd immunity required to starve these respiratory viruses out of existence. That’s one of several reasons why flu vaccines don’t provide long-lasting immunity and have to be repeated annually ― our immune system constantly needs to be updated to keep pace with the inevitable evolution of countless unnamed “variants.”
This never-ending conveyor belt of mutations means that everyone’s immunity to COVID was always only going to be temporary and only offer partial cross-reactive protection against future re-infections. Thus, from day one, COVID vaccination was always doomed to the same fate as the flu vaccine ― a lifelong regimen of annual booster shots to try to keep pace with “variants” for those unwilling to expose themselves to the risk of a natural infection. And the hope that by the time the vaccines (and their booster shots) roll off the production line, they won’t already be out of date when confronted by the current generation of virus mutations.
Genetic drift caused by mutations is much slower in viruses like measles, polio, or smallpox, which is why herd immunity can be used to control these other viruses (or even eradicate them as in the case of smallpox or polio). The reason the common respiratory viruses have such rapid genetic drift compared to these other viruses has much less to do with how many errors are produced during the copying process and much more to do with how many of those “imperfect” copies are actually able to survive and produce more copies.
A simple virus with an uncomplicated attack strategy for taking over host cells can tolerate a lot more mutations than a complex virus with a complicated attack strategy. Complexity and specialization put limits on how many of those imperfect copies have a chance at becoming successful mutations. Simple machinery doesn’t break down as easily if there is an imperfection in the mechanical parts. Complicated high-tech machinery will simply not work if there are even minor flaws in precision parts.
For example, before a virus can hijack the DNA of a host cell to begin making copies of itself, the virus needs to unlock the cell wall to gain entry. Cellular walls are made of proteins and are coated by sugars; viruses need to find a way to create a doorway through that protein wall. A virus like influenza uses a very simple strategy to get inside ― it locks onto one of the sugars on the outside of the cell wall in order to piggyback a ride as the sugar is absorbed into the cell (cells use sugar as their energy source). It’s such a simple strategy that it allows the influenza virus to go through lots of mutations without losing its ability to gain entry to the cell. Influenza’s simplicity makes it very adaptable and allows many different types of mutations to thrive as long as they all use the same piggyback entry strategy to get inside host cells.
By contrast, something like the measles virus uses a highly specialized and very complicated strategy to gain entry to a host cell. It relies on very specialized surface proteins to break open a doorway into the host cell. It’s a very rigid and complex system that doesn’t leave a lot of room for errors in the copying process. Even minor mutations to the measles virus will cause changes to its surface proteins, leaving it unable to gain access to a host cell to make more copies of itself. Thus, even if there are lots of mutations, those mutations are almost all evolutionary dead ends, thus preventing genetic drift. That’s one of several reasons why both a natural infection and vaccination against measles creates lifetime immunity ― immunity lasts because new variations don’t change much over time.
Most RNA respiratory viruses have a high rate of genetic drift because they all rely on relatively simple attack strategies to gain entry to host cells. This allows mutations to stack up quickly without becoming evolutionary dead ends because they avoid the evolutionary trap of complexity.
Coronaviruses use a different strategy than influenza to gain access to host cells. They have proteins on the virus surface (the infamous S-spike protein, the same one that is mimicked by the vaccine injection), which latches onto a receptor on the cell surface (the ACE2 receptor) ― a kind of key to unlock the door. This attack strategy is a little bit more complicated than the system used by influenza, which is probably why genetic drift in coronaviruses is slightly slower than in influenza, but it is still a much much simpler and much less specialized system than the one used by measles. Coronaviruses, like other respiratory viruses, are therefore constantly producing a never-ending conveyor belt of “variants” that make long-lasting herd immunity impossible. Variants are normal. The alarm raised by our public health authorities about “variants” and the feigned compassion of pharmaceutical companies as they rush to develop fresh boosters capable of fighting variants is a charade, much like expressing surprise about the sun rising in the East.
Once you got immunity to smallpox, measles, or polio, you had full protection for a few decades and were protected against severe illness or death for the rest of your life. But for fast-mutating respiratory viruses, including coronaviruses, within a few months they are sufficiently different that your previously acquired immunity will only ever offer partial protection against your next exposure. The fast rate of mutation ensures that you never catch the exact same cold or flu twice, just their closely related constantly evolving cousins. What keeps you from feeling the full brunt of each new infection is cross-reactive immunity, which is another part of the story of how you are being conned, which I will come back to shortly.
Blind Faith in Central Planning: The Fantasy of Timely Doses
But let’s pretend for a moment that a miraculous vaccine could be developed that could give us all 100% sterilizing immunity today. The length of time it takes to manufacture and ship 8 billion doses (and then make vaccination appointments for 8 billion people) ensures that by the time the last person gets their last dose, the never-ending conveyor belt of mutations will have already rendered the vaccine partially ineffective. True sterilizing immunity simply won’t ever happen with coronaviruses. The logistics of rolling out vaccines to 8 billion people meant that none of our vaccine makers or public health authorities ever could have genuinely believed that vaccines would create lasting herd immunity against COVID.
So, for a multitude of reasons, it was a deliberate lie to give the public the impression that if enough people take the vaccine, it would create lasting herd immunity. It was 100% certain, from day one, that by the time the last dose is administered, the rapid evolution of the virus would ensure that it would already be time to start thinking about booster shots. Exactly like the flu shot. Exactly the opposite of a measles vaccine. Vaccines against respiratory viruses can never provide anything more than a temporary cross-reactive immunity “update” ― they are merely a synthetic replacement for your annual natural exposure to the smorgasbord of cold and flu viruses. Immunity as a service, imposed on society by trickery. The only question was always, how long between booster shots? Weeks, months, years?
Spiked: The Fantasy of Preventing Infection
The current crop of COVID vaccines was never designed to provide sterilizing immunity – that’s not how they work. They are merely a tool designed to teach the immune system to attack the S-spike protein, thereby priming the immune system to reduce the severity of infection in preparation for your inevitable future encounter with the real virus. They were never capable of preventing infection, nor of preventing spread. They were merely designed to reduce your chance of being hospitalized or dying if you are infected. As former FDA commissioner Scott Gottlieb, who is on Pfizer’s board, said: “the original premise behind these vaccines were [sic] that they would substantially reduce the risk of death and severe disease and hospitalization. And that was the data that came out of the initial clinical trials.” Every first-year medical student knows that you cannot get herd immunity from a vaccine that does not stop infection.
In other words, by their design, these vaccines can neither stop you from catching an infection nor stop you from transmitting the infection to someone else. They were never capable of creating herd immunity. They were designed to protect individuals against severe outcomes if they choose to take them – a tool to provide temporary focused protection for the vulnerable, just like the flu vaccine. Pushing for mass vaccination was a con from day one. And the idea of using vaccine passports to separate the vaccinated from the unvaccinated was also a con from day one. The only impact these vaccine passports have on the pandemic is as a coercive tool to get you to roll up your sleeve. Nothing more.
Antibodies, B-Cells, and T-Cells: Why Immunity to Respiratory Viruses Fades So Quickly
There are multiple interconnected parts to why immunity to COVID, or any other respiratory virus, is always only temporary. Not only is the virus constantly mutating but immunity itself fades over time, not unlike the way our brains start forgetting how to do complicated math problems unless they keep practicing. This is true for both immunity acquired through natural infection and immunity acquired through vaccination.
Our immune systems have a kind of immunological memory ― basically, how long does your immune system remember how to launch an attack against a specific kind of threat. That memory fades over time. For some vaccines, like diphtheria and tetanus, that immunological memory fades very slowly. The measles vaccine protects for life. But for others, like the flu vaccine, that immunological memory fades very quickly.
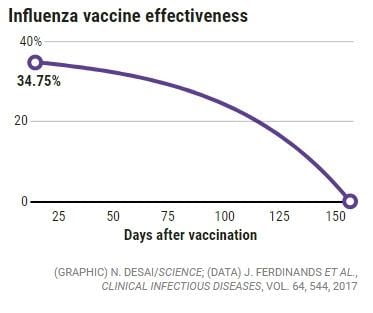
On average, the flu vaccine is only about 40% effective to begin with. And it begins to fade almost immediately after vaccination. By about 150 days (5 months), it reaches zero.
The solution to this strange phenomenon lies in the different types of immune system responses that are triggered by a vaccine (or by exposure to the real thing through a natural infection). This has big implications for coronavirus vaccines, but I’ll get to that in a moment. First a little background information…
A good analogy is to think of our immune system like a medieval army. The first layer of protection began with generalists – guys armed with clubs that would take a swing at everything – they were good for keeping robbers and brigands at bay and for conducting small skirmishes. But if the attack was bigger, then these generalists were quickly overwhelmed, serving as arrow fodder to blunt the attack on the more specialized troops coming up behind them. Spearmen, swordsmen, archers, cavalry, catapult operators, siege tower engineers, and so on. Each additional layer of defense has a more expensive kit and takes ever greater amounts of time to train (an English longbowman took years to build up the necessary skill and strength to become effective). The more specialized a troop is, the more you want to hold them back from the fight unless it’s absolutely necessary because they are expensive to train, expensive to deploy, and make a bigger mess when they fight that needs to be cleaned up afterwards. Always keep your powder dry. Send in the arrow fodder first and slowly ramp up your efforts from there.
Our immune system relies on a similar kind of layered system of defense. In addition to various non-specific rapid response layers that take out the brigands, like natural killer cells, macrophages, mast cells, and so on, we also have many adaptive (specialized) layers of antibodies (i.e. IgA, IgG, IgM immunoglobulin) and various types of highly specialized white blood cells, like B-cells and T-cells. Some antibodies are released by regular B-cells. Others are released by blood plasma. Then there are memory B-cells, which are capable of remembering previous threats and creating new antibodies long after the original antibodies fade away. And there are various types of T-cells (again with various degrees of immunological memory), like natural killer T-cells, killer T-cells, and helper T-cells, all of which play various roles in detecting and neutralizing invaders. In short, the greater the threat, the more troops are called into the fight.
This is clearly a gross oversimplification of all the different interconnected parts of our immune system, but the point is that a mild infection doesn’t trigger as many layers whereas a severe infection enlists the help of deeper layers, which are slower to respond but are much more specialized in their attack capabilities. And if those deeper adaptive layers get involved, they are capable of retaining a memory of the threat in order to be able to mount a quicker attack if a repeat attack is recognized in the future. That’s why someone who was infected by the dangerous Spanish Flu in 1918 might still have measurable T-cell immunity a century later but the mild bout of winter flu you had a couple of years ago might not have triggered T-cell immunity, even though both may have been caused by versions of the same H1N1 influenza virus.
As a rule of thumb, the broader the immune response, the longer immunological memory will last. Antibodies fade in a matter of months, whereas B-cell and T-cell immunity can last a lifetime.
Another rule of thumb is that a higher viral load puts more strain on your immune defenses, thus overwhelming the rapid response layers and forcing the immune system to enlist the deeper adaptive layers. That’s why nursing homes and hospitals are more dangerous places for vulnerable people than backyard barbecues. That’s why feedlot cattle are more vulnerable to viral diseases than cattle on pasture. Viral load matters a lot to how easily the generalist layers are overwhelmed and how much effort your immune system has to make to neutralize a threat.
Where the infection happens in the body also matters. For example, an infection in the upper respiratory tract triggers much less involvement from your adaptive immune system than when it reaches your lungs. Part of this is because your upper respiratory tract is already heavily preloaded with large numbers of generalist immunological cells that are designed to attack germs as they enter, which is why most colds and flus never make it deeper into the lungs. The guys with the clubs are capable of handling most of the threats that try to make through the gate. Most of the specialized troops hold back unless they are needed.
Catching a dangerous disease like measles produces lifetime immunity because an infection triggers all the deep layers that will retain a memory of how to fight off future encounters with the virus. So does the measles vaccine. Catching a cold or mild flu generally does not.
From an evolutionary point of view, this actually makes a lot of sense. Why waste valuable resources developing long-lasting immunity (i.e. training archers and building catapults) to defend against a virus that did not put you in mortal danger. A far better evolutionary strategy is to evolve a narrower generalist immune response to mild infections (i.e. most cold and flu viruses), which fades quickly once the threat is conquered, but invest in deep long-term broad-based immunity to dangerous infections, which lasts a very long time in case that threat is ever spotted on the horizon again. Considering the huge number of threats our immune systems face, this strategy avoids the trap of spreading immunological memory too thin. Our immunological memory resources are not limitless – long-term survival requires prioritizing our immunological resources.
The take-home lesson is that vaccines will, at best, only last as long as immunity acquired through natural infection and will often fade much faster because the vaccine is often only able to trigger a partial immune response compared to the actual infection. So, if the disease itself doesn’t produce a broad-based immune response leading to long-lasting immunity, neither will the vaccine. And in most cases, immunity acquired through vaccination will begin to fade much sooner than immunity acquired through a natural infection. Every vaccine maker and public health official knows this despite bizarrely claiming that the COVID vaccines (based on re-creating the S-protein spike instead of using a whole virus) would somehow become the exception to the rule. That was a lie, and they knew it from day one. That should set your alarm bells ringing at full throttle.
So, with this little bit of background knowledge under our belts, let’s look at what our public health officials and vaccine makers would have known in advance about coronaviruses and coronavirus vaccines when they told us back in the early Spring of 2020 that COVID vaccines were the path back to normality.
From a 2003 study: “Until SARS appeared, human coronaviruses were known as the cause of 15–30% of colds… Colds are generally mild, self-limited infections, and significant increases in neutralizing antibody titer are found in nasal secretions and serum after infection. Nevertheless, some unlucky individuals can be reinfected with the same coronavirus soon after recovery and get symptoms again.”
In other words, the coronaviruses involved in colds (there were four human coronaviruses before SARS, MERS, and COVID) all trigger such a weak immune response that they do not lead to any long-lasting immunity whatsoever. And why would they if, for most of us, the threat is so minimal that the generalists are perfectly capable of neutralizing the attack.
We also know that immunity against coronaviruses is not durable in other animals either. As any farmer knows well, cycles of reinfection with coronaviruses are the rule rather than the exception among their livestock (for example, coronaviruses are a common cause of pneumonia and various types of diarrheal diseases like scours, shipping fever, and winter dysentery in cattle). Annual farm vaccination schedules are therefore designed accordingly.
The lack of long-term immunity to coronaviruses is well documented in veterinary research among cattle, poultry, deer, water buffalo, etc. Furthermore, although animal coronavirus vaccines have been on the market for many years, it is well known that “none are completely efficacious in animals“. So, like the fading flu vaccine profile I showed you earlier, none of the animal coronavirus vaccines are capable of providing sterilizing immunity (none were capable of stopping 100% of infections, without which you can never achieve herd immunity) and the partial immunity they offered is well known to fade rather quickly.
What about immunity to COVID’s close cousin, the deadly SARS coronavirus, which had an 11% case fatality rate during the 2003 outbreak? From a 2007 study: “SARS-specific antibodies were maintained for an average of 2 years… SARS patients might be susceptible to reinfection >3 years after initial exposure.” (Bear in mind that, as with all diseases, re-infection does not mean you are necessarily going to get full-blown SARS; fading immunity after a natural infection tends to offer at least some level of partial protection against severe outcomes for a considerable amount of time after you can already be reinfected and spread it to others – more on that later.)
And what about MERS, the deadliest coronavirus to date, which made the jump from camels in 2012 and had a fatality rate of around 35%? It triggered the broadest immune response (due to its severity) and also appears to trigger the longest lasting immunity as a result (> 6yrs)
Thus, to pretend that there was any chance that herd immunity to COVID would be anything but short-lived was dishonest at best. For most people, immunity was always going to fade quickly. Just like what happens after most other respiratory virus infections. By February 2020, the epidemiological data showed clearly that for most people COVID was a mild coronavirus (nowhere near as severe than SARS or MERS), so it was virtually a certainty that even the immunity from a natural infection would fade within months, not years. It was also a certainty that vaccination was therefore, at best, only ever going to provide partial protection and that this protection would be temporary, lasting on the order of months. This is a case of false and misleading advertising if there ever was one.
If I can allow my farming roots to shine through for a moment, I’d like to explain the implications of what was known about animal coronaviruses vaccines. Baby calves are often vaccinated against bovine coronaviral diarrhea shortly after birth if they are born in the spring mud and slush season, but not if they are born in midsummer on lush pastures where the risk of infection is lower. Likewise, bovine coronavirus vaccines are used to protect cattle before they face stressful conditions during shipping, in a feedlot, or in winter feed pens. Animal coronavirus vaccines are thus used as tools to provide a temporary boost in immunity, in very specific conditions, and only for very specific vulnerable categories of animals. After everything I’ve laid out so far in this text, the targeted use of bovine coronavirus vaccines should surprise no-one. Pretending that our human coronavirus vaccines would be different was nonsense.
The only rational reason why the WHO and public health officials would withhold all that contextual information from the public as they rolled out lockdowns and held forth vaccines as an exit strategy was to whip the public into irrational fear in order to be able to make a dishonest case for mass vaccination when they should have, at most, been focused on providing focused vaccination of the most vulnerable only. That deception was the Trojan Horse to introduce endless mass booster shots as immunity inevitably fades and as new variants replace old ones.
Now, as all the inevitable limitations and problems with these vaccines become apparent (i.e. fading of vaccine-induced immunity, vaccines proving to only be partially effective, the rise of new variants, and the vaccinated population demonstrably catching and spreading the virus ― a.k.a. the leaky vaccine phenomenon), the surprise that our health authorities are showing simply isn’t credible. As I have shown you, all this was 100% to be expected. They intentionally weaponized fear and false expectations to unleash a fraudulent bait-and-switch racket of global proportions. Immunity on demand, forever.
Manufacturing Dangerous Variants: Virus Mutations Under Lockdown Conditions — Lessons from the 1918 Spanish Flu
At this point you may be wondering, if there is no lasting immunity from infection or vaccination, then are public health officials right to roll out booster shots to protect us from severe outcomes even if their dishonest methods to get us to accept them were unethical? Do we need a lifetime regimen of booster shots to keep us safe from a beast to which we cannot develop durable long-term immunity?
The short answer is no.
Contrary to what you might think, the rapid evolution of RNA respiratory viruses actually has several important benefits for us as their involuntary hosts, which protects us without the benefit of broad lifelong immunity. One of those benefits has to do with the natural evolution of the virus towards less dangerous variants. The other is the cross-reactive immunity that comes from frequent re-exposure to closely related “cousins”. I’m going to peel apart both of these topics in order to show you the remarkable system that nature designed to keep us safe… and to show you how the policies being forced on us by our public health authorities are knowingly interfering with this system. They are creating a dangerous situation that increases our risk to other respiratory viruses (not just to COVID) and may even push the COVID virus to evolve to become more dangerous to both the unvaccinated and the vaccinated. There are growing signs that this nightmare scenario has already begun.
Let’s start with the evolutionary pressures that normally drive viruses towards becoming less dangerous over time. A virus depends on its host to spread it. A lively host is more useful than a bedridden or dead one because a lively host can spread the virus further and will still be around to catch future mutations. Viruses risk becoming evolutionary dead ends if they kill or immobilize their hosts. Plagues came, killed, and then were starved out of existence because their surviving hosts had all acquired herd immunity. Colds come and go every year because their hosts are lively, easily spread the viruses around, and never acquire long-lasting immunity so that last year’s hosts can also serve as next year’s hosts ― only those who have weak immune systems have much to worry about. In other words, under normal conditions, mutations that are more contagious but less deadly have a survival advantage over less contagious and more deadly variations.
From the virus’ point of view, the evolutionary golden mean is reached when it can easily infect as many hosts as possible without reducing their mobility and without triggering long-term immunity in most of their hosts. That’s the ticket to setting up a sustainable cycle of reinfection, forever. Viruses with slow genetic drift and highly specialized reproductive strategies, like polio or measles, can take centuries or longer to become less deadly and more contagious; some may never reach the relatively harmless status of a cold or mild flu virus (by harmless I mean harmless to the majority of the population despite being extremely dangerous to those with weak or compromised immune systems). But for viruses with fast genetic drift, like respiratory viruses, even a few months can make a dramatic difference. Rapid genetic drift is one of the reasons why the Spanish Flu stopped being a monster disease, but polio and measles haven’t. And anyone with training in virology or immunology understands this!
We often speak of evolutionary pressure as though it forces an organism to adapt. In reality, a simple organism like a virus is utterly blind to its environment — all it does is blindly produce genetic copies of itself. “Evolutionary pressure” is actually just a fancy way of saying that environmental conditions will determine which of those millions of copies survives long enough to produce even more copies of itself.
A human adapts to its environment by altering its behaviour (that’s one type of adaptation). But the behaviour of a single viral particle never changes. A virus “adapts” over time because some genetic copies with one set of mutations survive and spread faster than other copies with a different set of mutations. Adaptation in viruses has to be seen exclusively through the lens of changes from one generation of virus to the next based on which mutations have a competitive edge over others. And that competitive edge will vary depending on the kinds of environmental conditions a virus encounters.
So, fear mongering about the Delta variant being even more contagious leaves out the fact that this is exactly what you would expect as a respiratory virus adapts to its new host species. We would expect new variants to be more contagious but less deadly as the virus fades to become just like the other 200+ respiratory viruses that cause common colds and flus.
That’s also why the decision to lock down the healthy population is so sinister. Lockdowns, border closures, and social distancing rules reduced spread among the healthy population, thus creating a situation where mutations produced among the healthy would become sufficiently rare that they might be outnumbered by mutations circulating among the bedridden. Mutations circulating among the healthy are, by definition, going to be the least dangerous mutations since they did not make their hosts sick enough to confine them to bedrest. That’s precisely the variants you want to spread in order to drown out competition from more dangerous mutations.
A host stuck in bed with a fever and not out dining with friends is limited in his ability to infect others compared to a host infected with a variety that only gives its host a sniffle. Not all bedridden hosts have caught a more dangerous mutation, but all dangerous mutations will be found among the bedridden. Thus as time goes by, dangerous mutations can only compete with less dangerous mutations if the entire population is limited in its ability to mix and mingle.
As long as the majority of infections are among the healthy, the more dangerous variants circulating among some of the bedridden will be outnumbered and will become evolutionary dead ends. But when public health officials intentionally restricted spread among the young, strong, and healthy members of society by imposing lockdowns, they created a set of evolutionary conditions that risked shifting the competitive evolutionary advantage from the least dangerous variants to more dangerous variants. By locking us all up, they risked making the virus more dangerous over time. Evolution doesn’t sit around to wait for you while you develop a vaccine.
Let me give you a historical example to demonstrate that this rapid evolution of a virus towards either more or less dangerous variants isn’t mere theory. Small changes to the environment can lead to very rapid changes in the virus’ evolution. The first wave of the 1918 Spanish Flu was not particularly deadly, with mortality rates similar to regular seasonal flu. However, the second wave was not only much deadlier but, rather unusually, was particularly deadly to young people rather than just the old and the weak. Why would the second wave be the deadly one? And what would cause the virus to evolve so quickly to become both more deadly and better adapted to preying on young people? At first glance it would seem to defy all evolutionary logic.
The answer demonstrates just how sensitive a virus is to small changes in evolutionary pressure. The Spanish Flu spread in the midst of the lockdown-mimicking conditions of World War One. During the first wave, the virus found a huge population of soldiers trapped in the cold damp conditions of the trenches and a near endless supply of captive bedridden hosts in overflowing field hospitals. By the Spring of 1918, up to three-quarters of the entire French military and half of British troops had been infected. These conditions created two unique evolutionary pressures. On the one hand, it allowed variants that were well adapted to young people to emerge. But on the other hand, unlike normal times, the cramped conditions of trench warfare and field hospitals allowed dangerous variants that immobilize their hosts to spread freely with little competition from less dangerous variants that spread through lively hosts. The trenches and field hospitals became the virus incubators driving the evolution of variants.
Normally young people are predominantly exposed to less dangerous mutations because the healthiest do all the mingling while the bedridden stay home. But the lockdown conditions of war created conditions that erased the competitive advantage of less dangerous mutations that don’t immobilize their hosts, leading to the rise of more dangerous mutations.
Thanks to the end of the war, the lockdown-mimicking conditions also ended, thereby shifting the competitive advantage back to less dangerous mutations that could spread freely among the mobile healthy members of the population. The deadliness of the second wave of the 1918 Spanish Flu is inextricably linked to the First World War, and the end of the war is linked to the virus fading into the background of regular cold and flu season.
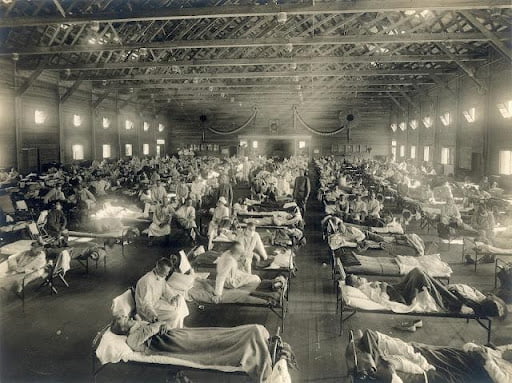
Soldiers from Fort Riley, Kansas, ill with Spanish flu at a hospital ward at Camp Funston
It is therefore highly likely that the 1918 Spanish Flu would never have been more than a really bad flu season had it not been for the amplifying effect of lockdown conditions created by a world at war.
It also raises the question, for which I don’t have an answer, whether the lockdown strategy during COVID was intentionally used to reduce spread among the healthy in order to keep the virus from fading into harmless irrelevancy. I use the word “intentionally” ― and it’s a strong word ― because the deadly second wave of the 1918 Spanish Flu and its causes are hardly secrets in the medical community. You’d have to be a completely reckless and utterly incompetent idiot, or a cynical bastard with an agenda, to impose any strategy that mimics those virus-amplifying conditions. Yet that’s what our health authorities did. And what they continue to do, while shamelessly hyperventilating about the risk of “variants” to force us to submit to medical tyranny based on mandatory vaccines, never-ending booster shots, and vaccine passports that can turn off access to our normal lives. This is cynicism at its finest.
Leaky Vaccines, Antibody-Dependent Enhancement, and the Marek Effect
The experience of the 2nd wave of the 1918 Spanish Flu also raises another question: What kind of evolutionary pressures are being created by using a leaky vaccine?
A vaccine that provides sterilizing immunity prevents the vaccinated from being able to catch or transmit the virus. They become a dead end for the virus. However, as I’ve already mentioned, the current crop of COVID vaccines, which are meant to train the immune system to recognize the S-spike proteins, were not designed to create sterilizing immunity. By their design, they merely help reduce the risk of severe outcomes by priming the immune system. The vaccinated can still catch and spread the virus ― the definition of a leaky vaccine ― and epidemiological data makes it very clear that this is now happening all around the world. Thus, both the vaccinated and the unvaccinated are equally capable of producing new variants. The idea that the unvaccinated are producing variants while the vaccinated are not is a boldfaced lie.
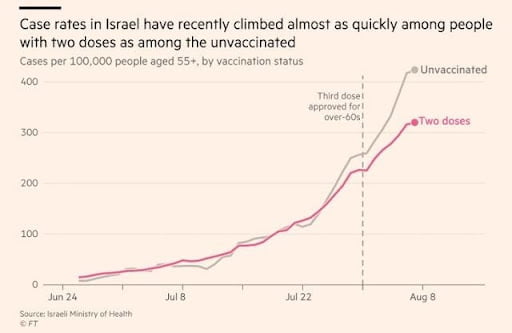
Source: “Israel hopes boosters can avert new lockdown as COVID vaccine efficacy fades.” August 23rd, 2021, Financial Times,
From an evolutionary perspective, this is a potentially dangerous scenario. What has been done by temporarily blunting the risk of hospitalization or death, but without stopping infection among the vaccinated, is to create a set of evolutionary conditions where a variant that is dangerous to the unvaccinated can spread easily among the vaccinated without making the vaccinated very sick. For lack of a better term, let’s call this a dual-track variant. Thus, because the vaccinated are not getting bedridden from this dual-track variant, they can continue to spread it easily, giving it a competitive advantage, even if it is highly dangerous to the unvaccinated.
Furthermore, since COVID vaccination only offers temporary short-term protection, as soon as immunity fades, the vaccinated themselves are also equally at risk of more severe outcomes. Thus, this creates the evolutionary pressure for the virus to behave as an increasingly contagious but relatively mild virus as long as everyone is vaccinated but as a dangerous but also very contagious virus as soon as temporary immunity wears off. The call for boosters every 6 months is already here. (Update: now it’s being revised down to 5 months.)
So, the pandemic really does have the potential to become the Pandemic of the Unvaccinated (the shameless term coined by public health officials to terrify the vaccinated into bullying their unvaccinated peers), but reality comes with a twist because if a dual-track variant does evolve it would be the unvaccinated (and those whose boosters have expired) who would have reason to fear the vaccinated, not the other way around as so many frightened citizens seem to believe. And the end result would be that we all become permanently dependent on boosters every 6 months, forever.
Hold on, you might say, the flu vaccine chart shown earlier also never provided sterilizing immunity. The flu vaccine is notoriously leaky but hasn’t gotten more dangerous, has it? The answer is complicated because the comparison is less useful than it first appears. As long as the majority of the population does not get the flu vaccine, more dangerous variants will face stiff competition from less dangerous ones circulating among the healthy unvaccinated population (average flu vaccination rates in most western countries are between 38-41%, with most other countries around the world doing very little vaccination against the flu).
And since the vaccine is only 40% effective to begin with and since immunity fades rapidly after the shot, the flu vaccine doesn’t provide much protection to begin with, thus reducing the chance that separate mutations would circulate among the vaccinated. And public health frequently gets the strain wrong (influenza has many strains that are constantly evolving so there is a lot of guesswork that goes into creating the right vaccine formula each year). In other words, lack of universal coverage and poor protection are likely preventing the emergence of a dual-track variant.
Furthermore, flu vaccination is not evenly distributed across the population. It is mostly the vulnerable and those who work around them that get it while children, young adults and other healthy members of society don’t get it. So, even if more deadly variants were to arise in nursing homes or hospital settings, the high number of healthy unvaccinated visitors to those facilities would constantly bring less deadly more contagious variants with them, thereby preventing more dangerous variants from gaining a competitive edge in nursing home or hospital settings. But if the leaky flu vaccinations were to be extended to everyone, or if nursing home populations continue to be kept isolated from the rest of society during COVID lockdowns, things might begin to look a little different.
However, what I am warning about is far from theoretical. There is a very clear example (well known to public health officials and vaccine developers) from the poultry farming industry where a universal leaky vaccine pushed a virus to evolve to become extremely deadly to unvaccinated chickens. It is called the Marek Effect. It began with a leaky vaccine that was rolled out to fight a herpes virus in industrialized high-density chicken barns. Vaccinated chickens were protected from severe outcomes but nevertheless continued to catch and spread the virus, so evolutionary pressure led to the emergence of a dual-track variant that become the dominant strain of this herpes virus. It continues to spread among the vaccinated chickens without killing them but kills up to 80% or more of unvaccinated birds if they get infected. Thus, a never-ending stream of vaccinations is now required just to maintain the status quo. I bet the pharmaceutical industry is smiling at all those drug-dependent chickens though — talk about having a captive audience!
It’s not a certainty that this will happen with the COVID vaccines, but the longer this fiasco continues and the higher that vaccination rates rise around the world, the more likely it becomes that we re-create the conditions for some kind of Marek effect to develop. A leaky vaccine used sparingly to protect small pockets of vulnerable individuals is very different than a leaky vaccine applied to everyone. The rapid change in behaviour of the 1918 Spanish Flu should be a warning to us all that a virus can adapt very quickly in response to small changes in evolutionary pressure. The closer we get to universal vaccination, the greater the danger that leaky vaccines will lead to dual-track variants that become more dangerous to the unvaccinated.
There is one other danger from leaky vaccines that is worth mentioning because researchers are already starting to see the first signs of it, as you can see discussed in this paper published on August 9th, 2021, in the Journal of Infection. It’s called antibody-dependent enhancement (ADE). It happens when a poorly designed vaccine trains antibodies to recognize a virus as an intruder without being strong enough to kill/neutralize them. Instead of the virus being neutralized inside the antibody when the antibody attacks and “swallows” it (antibodies envelope intruders in order to neutralize them), the virus takes over the antibody cell that attacked it and uses it as a host to start making copies of itself. Thus, the attacking antibody opens the door to the inside of the cell and becomes the virus’ unwitting host, thereby accelerating rather than stopping the infection.
Antibody-dependent enhancement is a well-documented phenomenon in attempts to develop vaccines against the RSV virus, dengue fever, and other coronaviruses. This is one of the reasons why previous attempts to develop a human coronavirus vaccine against the SARS virus failed. It kept happening in animal trials. And many doctors warned from day one that it would happen with these vaccines as well as new variants gradually emerge that are sufficiently different from the original variant upon which the vaccine is based. ADE doesn’t show up on the day after vaccination. It emerges gradually as new variants spread that are different from previous variants.
Quote from the aforementioned study: ADE may be a concern for people receiving vaccines based on the original Wuhan strain spike sequence (either mRNA or viral vectors). Under these circumstances, second generation vaccines with spike protein formulations lacking structurally-conserved ADE-related epitopes should be considered.
In other words, your previous vaccination protects you only until new variants arise, then the training that your previous vaccination gave your immune system becomes a liability as your immune system switches from protecting you to increasing your risk from the disease. Your only way to protect yourself is to dutifully get your next “updated” booster shot to protect you for next few short months. You become a permanent drug dependent vaccine customer. And you better hope next year’s formulation doesn’t get it wrong. And you better hope that updates can keep you safe indefinitely because there’s also the risk that updates will get less effective as the bad training from previous boosters begins to add up.
It puts a whole new spin on “trust the scientists.” Your life will literally be at their mercy.
I bet the pharmaceutical industry will be smiling at all those drug-dependent chickens loyal customers though — talk about having a captive audience! And what a sweet deal – vaccine makers have been granted an exemption from liability and, if it goes wrong, they are the go-to guy to solve it… with more boosters.
And with every booster, you’ll get to play Russian Roulette all over again with side effects: death, autoimmune diseases, reactivation of dormant viruses, neurological damage, blood clotting, and more. Here’s where the reported side effects on the US VAERS system stand at the time of writing (August 28th, 2021).
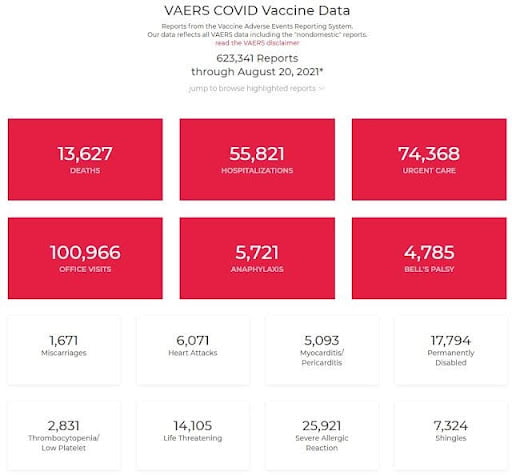
OpenVaers Search, August 28th, 2021
Leaky vaccines are playing with fire. All vaccine makers and public health authorities were aware of the potential for ADE with the development of a coronavirus vaccine. Yet they pushed for mass vaccination, from day one, without completing the long-term trials that are meant to rule out this kind of risk. They knowingly gambled with your future in their eagerness to get you onto your regimen of never-ending boosters and vaccine passports. Why not, if more boosters are the solution if something is going wrong. They can always blame it on the “variants.” The media won’t challenge them – not with billions of vaccine advertising dollars floating around.
Anti-Virus Security Updates: Cross-Reactive Immunity Through Repeated Exposure
And now we come to the second way in which our immune systems benefit from the rapid evolution of RNA respiratory viruses and to the sinister way in which public health policy is interfering with that system.
The once deadly 1918 Spanish Flu is still with us today; now it is part of the smorgasbord of viruses that cause colds and flus every winter precisely because subsequent variants evolved to be less deadly. As unpleasant as flu season is, for most of us it is not lethal unless we have weak or compromised immune systems. But each subsequent exposure teaches our immune system how to keep up with its gradual evolution over time.
In other words, each year’s fresh exposure to the latest strain of cold or flu virus functions as a sort of antivirus security update to partially prepare you for the next one. Fading immunity and changing mutations means you’ll never be 100% immune to the next one, but as long as updates are frequent enough, you’ll also never have 0% immunity. There will always be enough carry-over to protect you from the most serious outcomes unless you are unfortunate enough to have a weak immune system. That is why it is called cross-reactive immunity.
A broad smorgasbord of viruses cruising around during cold and flu season makes it less likely that we will die or get seriously ill when exposed to some new “variant” from London, India, or Brazil, or if we are exposed to a new “cousin”, like COVID, which crawls out of some bat cave or wet market or escapes from some lab in Wuhan.
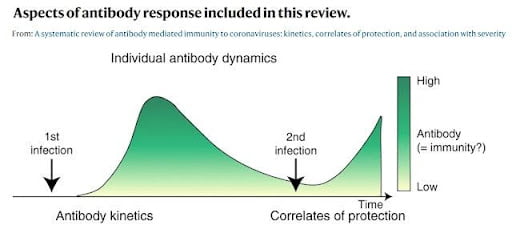
Partial cross-reactive immunity requires periodic re-exposure. Modified from Nature, 4704, September 17th, 2020.
But when we think about it for a moment, what was once dangerous when it was new soon becomes our most important ally for the future to protect us from the next dangerous new thing. As long as we are re-exposed frequently, before immunity fades to zero, cross-reactive immunity is the only realistic evolutionary strategy that humans have to protect us from the next viral variant or viral cousin of these fast-mutating respiratory viruses.
With sufficient leftover cross-reactive immunity from your last exposure, exposure to the latest variant of a virus may simply result in your immune system getting updated without you even noticing a single thing. That’s what it means to get an “asymptomatic” infection. Before we started tormenting the healthy with never-ending PCR tests to make us aware of all these “asymptomatic infections”, we were constantly getting lots of these “antivirus security updates” each time we encountered one of the more than 200 respiratory viruses circulating among us, often without even noticing the “infection”.
Many of these encounters are asymptomatic because our immune systems are able to neutralize them without even ruffling enough layers of our defenses to trigger any symptoms. Almost everyone gets a few immune system updates to the viruses that cause common colds, every single year, yet only a small percentage will ever get very sick. The rest may barely get a runny nose, or nothing symptoms at all.
Mass PCR testing during COVID created a massive freak-out over every single asymptomatic COVID update when we should have only been focused on those people who come down with severe symptomatic disease. There was never any justifiable reason to roll out PCR tests to asymptomatic citizens other than to heighten fear in the population in order to make them receptive to mass vaccination.
So, in a sense, those 201 respiratory viruses that cause our colds and flus are not just an inconvenience, they are nature’s solution to software updates ― even though they are dangerous to those with weak immune systems, for the rest of us our immune systems depend on them to give us partial protection against new strains that emerge through mutation or when new strains jump across species boundaries. Getting rid of those already circulating in society would make us more vulnerable to new variants that emerge. Adding another 200 will make us even safer once we get our first contact behind us.
Eradicating a relatively benign respiratory virus is therefore not a desirable goal. But making it fade into the background is a desirable public health goal so that what was once dangerous can now keep protecting us against the next one through cross-reactive immunity. Focused protection for the vulnerable, not lockdowns, was always the only realistic public health response to this respiratory virus, unless someone wanted to seize the opportunity as a way to rope the public into mass vaccinations.
Nature evolved this fascinating strategy of self-updating immunological countermeasures by continually testing us with mild versions of previous closely related respiratory viruses. Our immune system is therefore somewhat similar to an Olympic weightlifter whose muscles not only stay strong but get even stronger by routinely putting his muscles under a little bit of stress. Our immune system functions the same way ― it must be continually stress-tested with mild challenges to these fast-mutating viruses in order to develop the robust arsenal of defenses to keep us safe. It is a concept called anti-fragility, which was described in detail by Nassim Taleb in his ground-breaking book, Antifragile: Things That Gain from Disorder. Once you understand this concept, your fear of “variants” will rapidly dissolve.
The eradication of these fast-mutating respiratory viruses is therefore not just unachievable, it would actually be dangerous if we succeeded because it would eliminate the security updates that we need to protect us against new variants that crawl out of bat caves or jump species boundaries. This year’s runny nose is your protection against COVID-23. Your cross-reactive immunity to last years annoying flu might just save your life if something truly dangerous arrives, as long as it is at least somewhat related to what your immune system has seen before.
COVID could easily have turned out to be as dangerous to us as the Spanish Flu if it hadn’t been for the saving grace of cross-reactive immunity. As this study shows, up to 90-99% of us already had some level of protection to COVID thanks to partial cross-reactive immunity gained from exposure to other coronaviruses. The high percentage of infections that turn out to be asymptomatic bears that out.
Someone needs to remind Bill Gates, his fawning public health bootlickers, and the pharmaceutical companies that whisper sweet-nothings in his ear that in the natural world of respiratory viruses, most of us don’t need a regimen of never-ending booster shots to keep us safe from COVID variants ― we already have a perfectly functioning system to keep bringing us new updates. Respiratory viruses are a completely different beast than smallpox, polio, or measles; and pretending otherwise is not just silly, it’s criminal because anyone with a background in immunology knows better. But it’s a fantastic and very profitably way to scare a wide-eyed population into accepting never-ending booster shots as a replacement for the natural antivirus updates that we normally get from hugs and handshakes. Protect the vulnerable. Stop preying on the rest of us.
The Not-So-Novel Novel Virus: The Diamond Princess Cruise Ship Outbreak Proved We Have Cross-Reactive Immunity
A truly novel virus affects everyone because no-one has pre-existing cross-reactive partial immunity to it. That’s why the diseases that accompanied Christopher Columbus to the Americas killed up to 95% of North and South America’s indigenous populations (see Guns, Germs, and Steel, by Jared Diamond #Commissions Earned). To them, these diseases were novel because they had no previous exposure to them and therefore lacked the antivirus security updates acquired through pre-existing infections. They would have benefited greatly from access to a vaccine prior to first contact.
Thankfully, COVID-19 was not that kind of virus. Yet the media and public health officials shamelessly provoked fear that it was by using the scientifically accurate term novel to describe it, knowing full well that all scientists would understand this to mean a newly emergent strain while the general public would jump to the conclusion that this was an entirely new virus (also called a novel virus by scientists), like when tuberculosis or influenza accompanied Columbus to the Americas. This was a grotesque example of public health officials misusing scientific terminology, knowing full well that the public would misunderstand the term novel according to how we use the word in everyday language and not according to how the scientific community uses it.
That little game successfully sparked a wave of fear that is so strong that not only is everyone desperate for a leaky jab to lead them to safety, they are so scared that they won’t rest until all their friends, neighbors, and family members get one too, even if it requires extreme levels of coercion to get the job done. Canada has even recently gone as far as making vaccination mandatory for all federal employees, employees of Crown Corporations, employees of federally-regulated companies (i.e. utilities) and for all travellers on commercial airlines and trains (CBC, August 13th, 2021) !
Despite the scary numbers put out by the Chinese government in the early days of the pandemic, the outbreak on the Diamond Princess cruise ship served as an inadvertent petri-dish to study the COVID virus. Thanks to that example, by the end of February 2020, we knew that COVID was not some monster virus like the 1918 Spanish Flu but was simply another coronavirus strain that was closely related to previous coronaviruses and that most of us already carried some level of cross-reactive immunity to protect us.
How do we know that? The virus circulated freely onboard the ship, yet age corrected lethality remained between 0.025% and 0.625% (that’s on the order of a bad flu season and nothing at all like the fatality rate of the 1918 Spanish Flu, which was between 2% and 10%). Only 26% of the passengers tested positive for the virus and of those that tested positive 48% remained completely symptom free despite the advanced age of most of these passengers!
The Diamond Princess didn’t turn into the floating morgue of bygone eras when ships carrying a disease were forced into quarantine. That should have been the first clue that this virus was anything but novel in the colloquial understanding of the term. Like most cold and flu viruses, only those with weak immune systems were in danger while everyone else got off with little or no symptoms. That is simply not how a truly novel virus behaves when it encounters a population without any pre-existing cross-reactive immunity. The only plausible explanation for that lack of deadliness (deadly for some, annoying for some, and asymptomatic for most others) is that most people already have sufficient pre-existing cross-reactive immunity from exposure to other coronaviruses.
Research subsequently confirmed what the Diamond Princess outbreak revealed. As I mentioned before, studies like this one demonstrated that up to 90 – 99% of us already have some residual level of partial protection to COVID. And we also subsequently found out that most people who were exposed to the deadly SARS virus in 2003 have little to fear from COVID, again because of cross-reactive immunity. COVID was never a mortal threat to most of us.
The important thing to remember is that the Diamond Princess data was already publicly available since the end of February of 2020. Operation Warp Speed, the vaccine development initiative approved by President Trump, was nevertheless announced on April 29th, 2020. Thus, our health authorities knowingly and opportunistically recommended lockdowns and promoted vaccines as an exit strategy after it was already clear that the majority of us had some kind of protection through cross-reactive immunity. The Diamond Princess example provided the unequivocal proof that the only people who might benefit from a vaccine, even if it worked as advertised, were the small number of extremely vulnerable members of society with weak immune systems. Likewise, lockdowns should have been recommended only for nursing home residents (on a strictly voluntary basis to protect their human rights) while the pandemic surged through the rest of us.
The only plausible explanation for why our international health authorities ignored the example of the Diamond Princess is if they wanted to stoke fear among the public and if they wanted to bamboozle credible politicians in order to opportunistically achieve some other public health agenda. They pushed vaccination on everyone knowing full well that most people don’t need it and that protection would fade quickly even if the vaccines had been 100% effective, which they also knew was not going to be the case either. And yet they continue to push these vaccines using the same deceitful tactics even today. Water does not run uphill.
Mother Knows Best: Vitamin D, Playing in Puddles, and Sweaters
Just like during other cold and flu seasons, the vulnerable to COVID are overwhelmingly those with compromised immune systems: those whose immune systems are shutting down as they approach death from old age and those whose immune systems are compromised due to severe pre-existing conditions that reduce immune function.
For everyone else with a strong immune system and cross-reactive immunity, we have little to fear from the virus and its never-ending stream of mutations unless our immune systems are temporarily suppressed through illness, environmental conditions, or nutritional deficiencies.
Your mother’s warnings about putting on a sweater, hat, and dry socks, tucking in your shirt to cover your kidneys, and not playing in puddles were not about preventing infection by a cold or flu, it was about preventing symptomatic infection. Research has demonstrated that getting chilled can temporarily suppress your immune system. Thus, getting chilled increases the chance that an infection leads to symptomatic disease rather than merely updating your immune system through an asymptomatic infection. Your sweater won’t prevent you from catching an infection. But it might prevent that infection from becoming a symptomatic disease. It could be the difference between experiencing nothing and ending up in bed with a fever.
In the same way, topping up on vitamin C and D, eating properly, getting enough rest, getting hugs from loved ones, adopting a positive attitude in life, and smiling when you see a rainbow are all strategies that help keep your immune system strong. They don’t prevent infection, but they might reduce your risk of a bad outcome.
Ask the staff in a nursing home what happens to their patients when any of these important ingredients is missing ― vitamin and nutrient deficiencies, poor sleep, loneliness, and depression lay out the welcome mat for the Grim Reaper. A temporarily suppressed immune system cannot mount an adequate immune response even when we do have cross-reactive immunity.
Our public health authorities also all know this. This is not a mystery. Yet, instead of promoting these strategies as ways in which people could reduce their risk to severe outcomes, they have systematically downplayed, ignored, or labeled these strategies as “fake news“. Maximize the risk of death. Then promote the vaccine as the exclusive path to safety. Criminal.
You cannot control other people forever to avoid getting exposed to a respiratory virus. COVID Zero is an authoritarian fantasy. But you can control your food, your sleep, and your attitude so that your immune system can mount the strongest attack it can muster. The odds are that you already have all the cross-reactive immunity you need to survive this virus without a hitch. Look inwards to find freedom from fear. Take good care of yourself. Go play in the sun with your friends. And listen to your mother —tuck in your shirt!
The Paradox: Why COVID-Zero Makes People More Vulnerable to Other Viruses
As is so often the case when politicians try to run our lives for us, the government response to COVID is not just wrong, it is actually making us more vulnerable, both to COVID and to other respiratory viruses. Depriving nursing home patients of their loved ones, locking them in isolation, locking people in their homes, shutting down gyms, driving us into depression, and paralysing us with fear and uncertainty ensures that our immune systems will be working at suboptimal levels. Broken marriages, children deprived of social contacts, insomnia, the remarkable surge in obesity that occurred during COVID, and so many other consequences of these ill begotten strategies all have a toll on our ability to mount a strong immune response when we are inevitably exposed to any respiratory viruses.
Equally devastating is that, by disrupting our normal social contacts, we have reduced how much training our immune system is getting through repeated exposure to other respiratory viruses. A computer that stops getting security updates becomes increasingly vulnerable to future versions of viruses. The same goes for our immune system. COVID is not the only risk. Remember, there are more than 200 other respiratory viruses that are also circulating. They may not be getting much attention and may be temporarily starved for hosts while we are cooped up at home, but they haven’t gone away. They are waiting. And when they find us, they find hosts whose antivirus security updates are out of date.
In other words, by breaking our ability to socialize with our peers, what was once relatively harmless is becoming more dangerous to us because our immune systems are out of practice. This isn’t some theoretical risk. We’re already beginning to see the fallout from that lack of updates, with deadly consequences.
For example, New Zealand was praised internationally for adopting a COVID-Zero policy and for the low COVID cases that resulted. But the lockdowns, social distancing measures, and border closures also had another effect ― there was a 99.9% reduction in flu cases and a 98% reduction in cases of the RSV virus. Sounds good, right? Not so fast…
Systems that depend on constant challenges to become antifragile will become fragile if those challenges stop happening. A tree that grows up sheltered from the wind will break when it is exposed to the storm.
Now New Zealand’s myopic focus on COVID as the one and only risk is coming home to roost. Its hospitals are overflowing with children. But they’re not being hospitalized by COVID. They are falling ill with RSV virus because of the “immunity debt” that built up from not being continually exposed to all the respiratory viruses that make up normal life. These children are, quite literally, the next wave of victims of COVID-Zero. Being cut off from normal life has left them fragile. Instead of praise, it now is becoming apparent that New Zealand’s authoritarian strongwoman, Jacinda Ardern, and her public health advisors ought to be standing trial for gross negligence for ignoring the long-established research about how our immune systems depend on continual exposure to respiratory viruses in order to stay healthy.
As long as our social contacts are restricted, we are all becoming increasing vulnerable to all these other respiratory viruses because of the “immunity debt” that has built up during lockdowns and social distancing rules. It turns out that handshakes and hugs are not just good for the soul. Our public health officials have blood on their hands for denying us our normal lives.
This heightened risk to other viruses isn’t an unexpected outcome; there were plenty of doctors who warned about precisely this risk as lockdowns were being imposed. For example, Dr. Dan Erickson and Dr Artin Massihi warned about this phenomenon back in May of 2020. YouTube censored their video. Yet they were citing long-established science that was uncontested until society collectively lost its mind in 2020.
Introducing Immunity as a Service – A Subscription-Based Business Model for the Pharmaceutical Industry
As you can see from everything I have laid out in this essay, this misbegotten vaccine-enabled fever dream was never a realistic solution to stop COVID. At best, if the vaccines worked as advertised, all they could ever have been was one tool among many to provide the vulnerable with focused protection while the rest of us went about our normal lives, largely unaffected by our periodic antivirus security updates through exposure to the natural virus.
COVID-Zero in all its variations was a fantasy.
But it was not an accidental fantasy.
Water does not run uphill.
Every single public health official in the world has the education to know that what they have been promoting, from day one, is gibberish. What I have laid out in this essay is pretty basic virology and immunology knowledge. Which raises a rather alarming question: how can any virologist, immunologist, vaccine maker, or public health official knowingly promote this lie?
Why is there such a blind obsession with getting us all to take a vaccine that most people do not need and that can never provide long-lasting herd immunity?
It’s no mystery why pea-brained politicians might fall for this fantasy; they are only as good as the advisors they listen to. And politicians are shameless opportunists, so it is not surprising that they are now exploiting the situation to increase their powers and to harness this emerging command-and-control economy in pursuit of their own ideological goals — redistribution, carbon net zero, social credit score systems, you name it. In this Orwellian world, if you have a podium and a utopian dream, the world is your oyster, at least as long as the band keeps playing and the pitchforks can be kept off the streets.
But our public health officials and international health organizations are trained to know better. Yet they nevertheless set this nightmare in motion in violation of all their own long-established pandemic planning guidelines. They know eradication is impossible. They know most of us already have cross-reactive immunity. They know most of us are healthy enough so that our immune systems will protect us against severe outcomes from this virus. They know about the negative consequences imposed on our immune systems when we are prevented from living normal lives. They know they are increasing our risk to other viruses by preventing us from socializing. It’s their job to know. And, as I have demonstrated, they have known since day one.
But what if a shameless pharmaceutical industry could manipulate public health policies by capturing politicians, policymakers, and public health agencies through generous donations? What if the boundaries between public health agencies, international public health organizations, and pharmaceutical companies have become blurred to such a degree that each benefits from reinforcing one another’s best interests? What if they have all come to believe that vaccines against respiratory viruses are the holy grail of public health (and of generous funding), even if they have to play fast and loose with the truth to get humanity to accept them and even if they have to do a little evil to achieve some imagined future “greater good”?
What if the revolving door between pharmaceutical companies, public health, and international health organizations has created a kind of blind groupthink within this holy trinity? What if anyone caught up in that system is forced to bite their tongue because to speak out is a deathblow to their career? What if many of those caught up in the system genuinely believe the lies, despite a lifetime of training that should tell them otherwise? The powerful effect of groupthink, demonstrated by the Ash Conformity Experiments, can make people blind to what is staring them in the face. Even the medieval kings knew they needed a court jester to prevent the king from growing a big head. But what if, in the hallowed halls of this holy trinity, all the court jesters have long since been purged or cowed into silence?
A quote that best sums up the thinking inside many of our public health institutions comes from Peter Daszak, head of EcoHealth Alliance, a non-profit non-governmental organization that works closely with public health agencies like the National Institutes of Health (NIH) and intergovernmental organizations like the WHO (published in a 2016 report by the National Academy of Sciences): “Daszak reiterated that, until an infectious disease crisis is very real, present, and at an emergency threshold, it is often largely ignored. To sustain the funding base beyond the crisis, he said, we need to increase public understanding of the need for MCMs [medical counter measures] such as a pan-influenza or pan-coronavirus vaccine. A key driver is the media, and the economics follow the hype. We need to use that hype to our advantage to get to the real issues. Investors will respond if they see profit at the end of process, Daszak stated.”
In the presence of so much conflict of interest, in the absence of the checks and balances provided by individual rights, in the censorious atmosphere of cancel culture that has infected all our public institutions, and with so many institutional donors (private and governmental alike) being enamored with social-engineering projects and blinded by their own arrogance, it would perhaps be more surprising if this vaccine-fueled hysteria hadn’t happened.
In view of the circumstances, what happened almost seems inevitable. To the eyes of profit-hungry pharmaceuticals and funding-hungry national and international public health institutions, this virus must look like manna from heaven. They must feel like a fox that has been invited into the henhouse by ripe chickens that are begging to be plucked.
History never repeats itself, but it does often rhyme. What has emerged during COVID is simply a bigger, better, bolder replay of what happened during the 2009 swine flu hysteria. I’d like to share a few quotes with you – and keep in mind that these are about the 2009 Swine Flu scandal, not COVID:
From a 2010 article entitled: European Parliament to Investigate WHO and “Pandemic” Scandal [Emphasis mine]:
- “In his official statement to the Committee, Wodarg criticized the influence of the pharma industry on scientists and officials of [the] WHO, stating that it has led to the situation where “unnecessarily millions of healthy people are exposed to the risk of poorly tested vaccines,” and that, for a flu strain that is “vastly less harmful” than all previous flu epidemics.”
- “For the first time, the WHO criteria for a pandemic was changed in April 2009 as the first Mexico cases were reported, to make not the actual risk of a disease but the number of cases of the disease [the] basis to declare “Pandemic.” By classifying the swine flu as [a] pandemic, nations were compelled to implement pandemic plans and also t[o] purchase swine flu vaccines.”
And here are a series of even more revealing quotes from a 2010 report published by Der Spiegel called: Reconstruction of a Mass Hysteria — The Swine Flu Panic of 2009:
- “Researchers in more than 130 laboratories in 102 countries are constantly on the lookout for new flu pathogens. Entire careers and institutions, and a lot of money, depend on the outcomes of their work. “Sometimes you get the feeling that there is a whole industry almost waiting for a pandemic to occur,” says flu expert Tom Jefferson, from an international health nonprofit called the Cochrane Collaboration. “And all it took was one of these influenza viruses to mutate to start the machine grinding.”
- “Does this mean that a very mild course of the pandemic was not even considered from the start? At any rate, efforts to downplay the risks were unwelcome, and the WHO made it clear that it preferred to base its decisions on a worst-case scenario.”We wanted to overestimate rather than underestimate the situation,” says Fukuda [Keiji Fukuda was the Assistant Director-General for Health, Security and Environment for the WHO at that time].”
- “The media also did its part in stoking fears. SPIEGEL, for example, had reported at length on the avian flu. Now it devoted a cover story to the new “global virus,” a story filled with concerns that the swine flu pathogen could mutate into a horrific virus.”
- “The pharmaceutical industry was particularly adept at keeping this vision alive.”
- “We expected a real pandemic, and we thought that it had to happen. There was no one who suggested re-thinking our approach.”
- “the vast majority of experts on epidemics automatically associate the term “pandemic” with truly aggressive viruses. On the WHO Web site, the answer to the question “What is a pandemic?” included mention of “an enormous number of deaths and cases of the disease” — until May 4, 2009. That was when a CNN reporter pointed out the discrepancy between this description and the generally mild course of the swine flu. The language was promptly removed.”
- “‘Sometimes some of us think that WHO stands for World Hysteria Organization,’ says Richard Schabas, the former chief medical officer for Canada’s Ontario Province.”
- “A party with strong connections in Geneva had a strong interest in phase 6 being declared as quickly as possible: the pharmaceutical industry.”
- “Meanwhile, a debate had erupted over whether Germany had chosen the wrong vaccine, Pandemrix [it was later found to have caused narcolepsy in some patients, which is an autoimmune disease]. It contained a new type of agent designed to boost its effectiveness, known as an adjuvant, which had never undergone large-scale human trials in connection with the swine flu antigen. Were millions of people about to receive a vaccine that had hardly been tested?”
- “But the contracts for Pandemrix had been signed in 2007, and they came into effect automatically when the WHO decided to declare phase 6.”
- “The ministers felt pressured from all sides. On the one hand, the media were stoking fears of the virus. The German tabloid newspaper Bild, in particular, was printing new tales of horror almost daily. On the other hand, the pharmaceutical companies were upping the pressure and constantly setting new ultimatums.”
- “Oct. 9, 2009: Wolf-Dieter Ludwig, an oncologist and chairman of the Drug Commission of the German Medical Association , says: ‘The health authorities have fallen for a campaign by the pharmaceutical companies, which were plainly using a supposed threat to make money.'”
- “Oct. 21, 2009: A BILD newspaper headline, printed in toxic yellow, warns: “Swine Flu Professor Fears 35,000 Dead in Germany !” The professor’s name is Adolf Windorfer, and when pressed, he admits that he has received payments from the industry, including GSK and Novartis. Next to the BILD headline is an ad for the German Association of Pharmaceutical Companies.”
- “According to Wodarg, the WHO’s classification of the swine flu as a pandemic have earned the pharmaceutical companies $18 billion in additional revenues. Annual sales of Tamiflu alone have jumped 435 percent, to €2.2 billion.”
Rinse and repeat in 2020-2021.
What if, upon recognizing the emergence of a new pandemic, those in the know opportunistically made vaccines the endgame? What if all the vaccine injuries recorded on VAERS and all the risks they are taking with our lives are simply collateral damage – a calculated investment risk – in order to turn their dream of subscription-based “immunity as a service” into reality.
In the words of Bill Gates, “we kind of caught mRNA half way to prime time.” Maybe we should believe him — and gape in awe at the recklessness and contempt they have shown for their fellow citizens in order to capitalize on this “window of opportunity”. Carpe diem (seize the day). Don’t sweat the small stuff. Keep your eye on the ball… and on the year-end bonuses.
What if COVID-Zero, in all its variations, was merely a strategy to herd us together so we obediently line up for an endless string of booster shots as a trade-off for access to our lives?
In other words, what if someone could bamboozle our leaders into believing that the only way back to a normal life is for vaccines to replace the role that hugs and handshakes used to play in order to update us with the latest antivirus security updates?
What if, by depriving us of normal life, those who stand to gain from vaccines can forever cement themselves at the center of society by providing an artificial replacement for what our immune systems used to do to protect us against common respiratory viruses back when we were still allowed to live normal lives?
The headlines tell the story:
- “Pfizer CEO says third Covid vaccine dose likely needed within 12 months.” (CNBC, April 15th, 2021)
- “Variants could be named after star constellations when Greek alphabet runs out, says WHO Covid chief.” (The Telegraph, August 7th, 2021)
- “Fauci warns Americans may face having booster shots indefinitely” (Daily Mail, August 13th, 2021, and Dr. Fauci in his own words on YouTube on August 12th, 2021)
- “Biden OKs booster shots 5 months after 2nd dose” (Boston Globe, August 27th, 2021)
What if the fast mutation of RNA viruses ensures that no vaccine will ever be fully effective at providing lasting immunity, thus creating the illusion that we are permanently in need of vaccine boosters?
What if politicians could be convinced to make vaccination mandatory in order to prevent potential customers from opting out?
What if, by relying on lockdowns during the winter season, our vulnerability to other viruses increased, which could then be used to rationalize expanding the jab, via mission creep, to simultaneously vaccinate us against RSV, influenza, other coronaviruses, the common cold, and so on, despite knowing full well that the protection that these vaccines offer against respiratory viruses is only temporary?
And what other social engineering goals can be rolled into your annual booster shot in the future once you are permanently bound to these annual jabs and vaccine passports? In an atmosphere of hysteria, it’s a system ripe for abuse by opportunists, ideologues, power hungry totalitarians, and Malthusian social engineers. The snowball doesn’t have to grow by design. Mission creep happens all on its own once Pandora’s Box is opened to coerced vaccinations and conditional rights. The road to Hell is frequently paved by good intentions… and hysteria.
So, what if COVID-Zero and the vaccine exit strategy is merely the global state-sanctioned equivalent of a drug dealer creating dependency among its customers to keep pushing more drugs?
What if it was all just a way of convincing society of the need for subscription-based “immunity as a service”? The subscription-based business model (or some version of it) is all the rage these days in the corporate world to create loyal captive audiences that generate reliable money streams, forever. Subscriptions are not just for your cable TV and gym membership anymore.
Everything has been redesignated as a “consumable”.
- Netflix did it with movies.
- Spotify did it with music.
- Microsoft did it with its Office suite.
- Adobe did it with the Photoshop editing suite.
- The smartphone industry did it with phones that need to be replaced every 3 to 5 years.
- The gaming industry did it with video games.
- Amazon is doing it with books (i.e. Kindle Unlimited).
- The food industry is doing it with meal delivery services (i.e. Hello Fresh).
- Uber is doing it with subscription-based ride sharing.
- Coursera is doing it with online education.
- Duolingo and Rosetta Stone are doing it with language learning.
- Zoom is doing it with online meetings.
- Monsanto and its peers did it to farmers with patented seed technology, which cannot legally be replanted, and is lobbying to try to legalize the use of terminator seed technology (GMO seeds that are sterile in the second generation to prevent replanting).
- The healthcare industry is doing it with concierge medical services, fitness tracking apps (Fitbit), sleep-tracking apps, and meditation apps.
- The investment industry is doing it with farmland, with investors owning the land and leasing it back to farmers in a kind of modern revival of the sharecropping system. (Bill Gates is the largest farmland owner in the USA – are you surprised?)
- Blackrock and other investment firms are currently trying to do it with homes to create a permanent class of renters.
And public health authorities and vaccine makers have been trying to do it with flu vaccines for years, but we’ve been stubbornly uncooperative. Not anymore.
Remember when the World Economic Forum predicted in 2016 that by 2030 all products would become services? And remember their infamous video in which they predicted that “You will own nothing. And you will be happy.”? Well, the future is here. This is what it looks like. The subscription-based economy. And apparently it now also includes your immune system in a trade-off for access to your life.
Let’s revisit the Peter Daszak quote from earlier. A second read allows the message to really hit home: “Daszak reiterated that, until an infectious disease crisis is very real, present, and at an emergency threshold, it is often largely ignored. To sustain the funding base beyond the crisis, he said, we need to increase public understanding of the need for MCMs [medical counter measures] such as a pan-influenza or pan-coronavirus vaccine. A key driver is the media, and the economics follow the hype. We need to use that hype to our advantage to get to the real issues. Investors will respond if they see profit at the end of process, Daszak stated.”
Isn’t it ironic that he didn’t even care which vaccine was pushed? Influenza or coronavirus, it made no difference. It was always about funding. It was always about the money. It always was. It always is.
The holy trinity of pharmaceutical companies, public health, and international health organizations, all egging each other on in their hunger for a reliable flow of cash: shareholder profits, larger budgets, and governmental donations. Their interests are perfectly aligned and the lines between them are blurred to such a degree that each benefits from reinforcing one another’s best interests.
And why would politicians and media bow to the holy trinity?
Big Pharma spent an average of US$4.7 billion per year between 1999 and 2018 on lobbying and campaign contributions, just in the USA!
Big Pharma also shells out $US20 billion each year to schmooze doctors and another US$6 billion on drug ads, just in the USA. So, it’s no surprise why legacy media and Big Tech are tripping over themselves not to ruffle the party line — they live and die by the almighty advertising dollar. Never bite the hand that feeds you.
So, they are all dancing to the same tune while your pocket gets picked and your arm gets pricked, and everyone wins… except you and me. We are the cow that gets milked. We are the serfs that fund their largesse in this neo-feudal society where a few big boys own the assets and everyone else is beholden to those above them in the hierarchy for access to, well, everything — land, resources, rights, individual autonomy, and even immune systems. My body, their choice.
What if, in an atmosphere of runaway hysteria, a police state founded on medical tyranny is creating itself, fueled by a toxic brew of self-serving opportunists who have seized the moment to superimpose their own goals on a fortuitous virus, until one day you wake up to find yourself chained and milked, like a cow in a dairy barn, under the absolute custody of a modern-day Louis the Fourteenth and his royal court full of drug pushers, ideologues, and militant devotees? The modern face of feudalism, updated for the 21st century.
And what if a society that has lost its principles, a society that is eager to hand over individual responsibility to “experts,” a society that is held hostage to cancel culture mobs, a society that no longer has transparency into the decisions made by its experts, a society led by a censorious political class full of immoral opportunists, a society that has fallen so in love with big government that red tape and cronyism have completely erased the self-limiting checks and balances of a free and open society, and a society that has elevated safety to a new sort of religious cult is a society that has no immunity to protect itself from predators who treat us like cattle?
No period in history has ever lacked in snake-oil salesmen, ideologues, and social engineers eager to take society for a ride. Most of the time, they are ignored. So, what if the only real mystery is why society has grown so willing to accept the collar and yoke?
What if all this really is just as simple as that?
The Path Forward: Neutralizing the Threat and Bullet-Proofing Society to Prevent This Ever Happening Again.
Now we know we’ve been played, how we’ve been played, and why we’ve been played. Again. Just like during the 2009 Swine Flu con. Only bigger, bolder, and better. They learned from their mistakes. We didn’t.
But now that you see the con, you can’t unsee it. And now that you understand the threat and how the game is being played, there is a weight that comes off your shoulders.
When you know there’s a threat, but you don’t know exactly what it is, every movement in the grass might be a tiger or a snake or a scorpion. It’s paralysing and exhausting to defend yourself against an invisible unknown and they have used that fear masterfully against us to keep us frozen. But once you spot the tiger in the grass, you know where to direct your focus, your feet become unglued, your voice becomes bold, and you regain the clarity of thought to defend yourself.
The con is clear. It’s time to focus all our might on stopping this runaway train before it takes us over the cliff into a police state of no return. Stand up. Speak out. Refuse to play along. Stopping this requires millions of voices with the courage to say NO — at work, at home, at school, at church, and out on the street.
“Nonviolent direct action seeks to create such a crisis & foster such a tension that a community which has constantly refused to negotiate is forced to confront the issue. It seeks so to dramatize the issue that it can no longer be ignored.” — Martin Luther King Jr.
Compliance is the glue that holds tyranny together. Non-compliance breaks it apart. One person alone cannot stop this. But if millions find the courage to raise their voices and the courage to refuse to participate in the system on these tyrannical medical terms, it will throw the system into such a crisis and create such a tension that the community will be forced to confront the issue. Without enough truckers, no-one eats. Without enough medical staff, hospitals close. Without enough workers, supply chains break. Without enough policemen, laws cannot be enforced. Without enough garbage collectors, cities grind to a halt. Without enough cashiers, box stores cannot stay open. Without enough administrators, institutions cease to function. Without enough staff, corporations lose profits. Without enough servers, restaurants cannot serve their customers. And without enough customers, businesses are brought to their knees.
Tyranny is not sustainable if the system grinds to a halt. Make it grind by being a thorn in everyone’s side until they give us back our freedoms and end this ridiculous charade. They are trying to impose vaccine passports and mandatory vaccinations. But we hold the cards… but only if we are bold enough to stand up even at the risk of finding ourselves standing alone. Courage begets courage. It was Martin Luther King’s secret power. It must be ours.
Now that you see the con, you also know the simple recipe to make this virus go away before their reckless policies turn it a monster virus for real. Remember 1918. End the war on the virus. Let the young folks come out of the trenches. Let people go back to their lives. Provide focused protection for the vulnerable. That is how this virus fades into the history books.
It’s time to be bold. It’s time to call out the fraudsters. And it’s time to reclaim the habits, values, and principles that are required to fix our democratic and scientific institutions to prevent this from ever happening again.
Feudalism was one giant stinking cesspool of self-serving corruption. Individual rights, free markets, the democratic process, and limited government were the antidotes that freed humanity from that hierarchical servitude. It seems we have come full circle. The COVID con is a symptom, not the cause, of a broken system.
Modern liberal democracy all around the world was inspired by the system of checks and balances that America’s Founding Fathers built to prevent government from being co-opted by the special interests of its leaders, institutions, corporations, and most influential citizens. The ink was barely dry when those principles began to be ignored by those with ever greater enthusiasm for an all-powerful referee to manage even the most intimate details of how everyone lives their lives. After two and a half centuries of effort the admirers of big government have achieved their heart’s desire. And what a glorious and rotten cesspool of self-serving corruption it is.
But the principles laid out in America’s Founding remain as true today as the day they were written and are waiting to be rediscovered. If there is one culprit who deserves to shoulder more blame than any other for the fiasco of the last 18 months, it is society itself for allowing itself to fall prey to the siren song of big government, the illusion that there can ever be a benevolent, virtuous, and incorruptible referee. He who creates the red tape, he who has the keys to the treasury, he who wields the power of the tax collector, and he who commands those sent to enforce the laws will always have an entourage of self-serving charlatans, rent seekers, and parasites following him wherever he goes. So, keep his powers on a very short leash to keep other people’s hands off your money, your property, your freedom, and your body. You don’t need better leaders. You need less powerful institutions. That’s how you prevent this from ever happening again.
Freedom of speech, individual rights, private property, individual ownership, competition, good faith debate, small government, minimal taxes, limited regulation, and free markets (the opposite of the crony capitalism we now suffer under), these are the checks and balances that bullet-proof a society against the soulless charlatans that fail upwards into positions of power in bloated government institutions and against the parasitic fraudsters that seek to attach themselves to the government’s teat.
Yes, we need a Great Reset. Just not the subscription-based version that the World Economic Forum imagined.
“One of the saddest lessons of history is this: If we’ve been bamboozled long enough, we tend to reject any evidence of the bamboozle. We’re no longer interested in finding out the truth. The bamboozle has captured us. It’s simply too painful to acknowledge, even to ourselves, that we’ve been taken. Once you give a charlatan power over you, you almost never get it back.” ― Carl Sagan, The Demon-Haunted World: Science as a Candle in the Dark.
This is an adapted except of the author’s book Autopsy of a Pandemic.
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








