
Every crisis, they say, is an opportunity. Governments, health bureaucrats and drug regulators all over the world have exploited the Covid-19 crisis to grab power and gain control over our lives. Predictably, rather than to most people’s surprise, many are proving singularly resistant to relinquishing their extraordinary powers, instead extending the emergency and broadening its scope to embrace other issues.
Efforts to control the pandemic narrative began with a systematic suppression of any suggestion that it might have originated in a research lab of the Wuhan Institute of Virology, then moved on to denigrate, silence and smear critics of lockdowns, masks and vaccine efficacy and mandates.
Australia’s Amended Health Practitioner Regulation National Law
The latest iteration in Australia occurred on October 13 when the Queensland Parliament amended the Health Practitioner Regulation National Law Act to fundamentally reshape the relationship between doctors, patients and health regulators. As per an existing intergovernmental agreement, the Queensland change will be replicated in cascading legislative amendments in other states and territories to ensure a uniform National Law.
On February 22, Australian federal and state health ministers had approved the Health Practitioner Regulation National Law Amendment Bill. The updates to the guiding principles included “an increase in the regulatory responses available to protect public safety.” At best, this is vague and ambiguous.
At worst, it shifts the balance decisively from the individual-centric in liberal democracies to the collective safetyism of technocrats and experts, justifying restrictions on individual rights and agency for the greater good as determined by government agencies. Doctors will be prohibited from expressing their opinion and using their experience, training, education and knowledge of the patient, if this contradicts what the health bureaucrats say is in the interests of “public confidence in safety.” The latter will remote-control how doctors should approach treatment recommendations for patients.
There were several submissions arguing against various elements of the amendment. The Australian Medical Association queried what a “main guiding principle” means “in practice” and argued that the “concept of public confidence is not always clear cut.” The Royal Australian College of General Practitioners submitted that the amendments would imbalance the system even further away from the protection of patient safety and toward “the prosecution of practitioners,” to the detriment of doctors’ confidence in the National Law.
The most substantial submission came from the Australian Medical Professionals Society and the Nurses Professional Association of Australia representing more than 10,000 health professionals. They expressed concern that “the broad and discretionary nature of claims to ‘public safety and confidence’” can be abused “as a mechanism to enforce compliance with government directives.” On the one hand, these could be disconnected from science and evidence.
On the other, they could be used to control health practitioners in direct “conflict with their ethical duties and code of conduct obligations.” They weren’t confident that the provisions for public health and safety would in fact either “improve public protection from clinical misconduct” or “increase confidence in the public health system.” Instead the proposed powers would “serve to conveniently silence voices of expertise that wish to correct health authorities” and prove counterproductive by preventing “necessary information and communication from entering the public sphere.”
Everything done by health bureaucrats and regulators since March 2020, in the name of ensuring public safety and stopping disinformation, indicates we should fear the worst and would be naive to hope for the best. This includes psychological manipulation of emotions and feelings to nudge people into compliance with health directives.
Long-standing principles that have guided Australian doctors and ensured its health system is second to none will be undermined: the Hippocratic Oath’s duty of “Do no harm,” informed consent of the patient based on a harm-benefit evaluation of different treatment options, the risks associated with them in the best professional judgment of the doctor, and the sanctity of the doctor-patient relationship.
People’s faith in their GPs could collapse once they realize doctors are barred from questioning putative benefits or pointing to possible risks of recommended treatments. Instead, they must stay within the boundaries laid down by bureaucrats and regulators, the latter often subject to industry capture.
California has passed a similar law empowering the state’s medical board to revoke the license of physicians who express opinions “contradicted by contemporary scientific consensus to the standard of care.” Or, as helpfully translated by the New York Post sub-editors: “California makes it illegal for doctors to disagree with politicians.”
The Debate on the Harm-Benefit Balance of Covid Vaccines
For health bureaucrats and regulators, the latter often with compromising links to industry, to claim a monopoly on scientific truth is scandalous. The effort to shut down legitimate debates on pain of excommunication from the medical profession represents a clear and present danger to public health.
Having overturned a hundred years of science and policy orthodoxy on pandemic management with Covid, we are intent on revolutionizing the everyday practice of medicine by subordinating the professional judgment of doctors on the best treatment options for their patients, to the directives of bureaucrats and health regulators. With public esteem for politicians at all-time lows, this is not likely to inspire confidence in the health service.
Consider globally contested opinion on the benefit-harm balance of Covid vaccines for children. Their risk of severe illness or death from Covid is tiny, of serious adverse reactions is higher and the long-term effects are unknown. On October 7, Florida issued a press release recommending against mRNA Covid vaccines for 18–39 year-old males. Their analysis had found an 84 percent higher risk of cardiac-related death within 28 days of vaccination in this group. Over-60s have a 10 percent increased risk.
This complements Florida’s guidance on paediatric vaccine guidance issued in March which recommends against Covid vaccines for healthy under-18s. They note the limited risk to infants and children of severe illness due to Covid, the high prevalence of existing immunity among them, reduced vaccine efficacy and “higher than anticipated” severe adverse events, including myocarditis.
Florida thus joins Denmark, Norway and Sweden in ending vaccine recommendations for 12–17 year-olds and also, in two of these, for under 50s and 65s. Albeit contested, there is a substantial and growing body of scientific studies that support their skepticism toward the net benefits of Covid vaccines for infants, children and adolescents.
Florida’s guidance includes three recommendations that are directly relevant to Australia’s National Law:
- People are encouraged to discuss all potential vaccine benefits and risks with their health care provider.
- The risk associated with mRNA vaccination should be weighed against that with Covid infection.
- Doctors should inform patients of the possible cardiac complications that can arise after receiving an mRNA vaccine.
Yet Australia’s Therapeutic Goods Administration has approved vaccines for children aged 6 months-5 years. Meanwhile, many of the claims advanced in support of the vaccines – they stop infection and transmission and prevent severe illness and death – have had to be abandoned one after another but were never “fact-checked” by social media platforms, while the early critics of these claims were assessed by the self-styled fact-checkers to be spreading disinformation and promoting conspiracy theories – until they aren’t any longer.
Moreover, people who die inside 14 days of a vaccine dose are wrongly classified as “unvaccinated.” This distorts the statistics on the net harm-benefit balance to an indeterminate degree. In a particularly egregious example, an article in Nature on September 23 explained that the authors (1) had classified unvaccinated and single-dose vaccinated into the one catch-all category of unvaccinated, and (2) unvaccinated individuals with previous infection had been classified as “fully vaccinated” (Supplementary Table 2).
This in a study whose main objective was to assess the comparative susceptibility to infection by the Omicron variant of the vaccinated versus the unvaccinated within Danish households in December 2021. They concluded that the vaccinated are less susceptible. I can empathize with the reaction of Julian Conradson that after such analytical legerdemain in a leading peer-reviewed journal, “Academia Is Dead.” Little wonder that a poll by the Pew Research Center in February mapped falling confidence in medical scientists since 2020.
Examples of Off-Limits Topics
Examples of studies that doctors could not discuss without fear of investigation and repercussions include:
- In a new study in preprint that looked at 31 pre-vaccination national seroprevalence studies to estimate the infection fatality rate (IFR) stratified by age, John Ioannidis and his team found that the average IFR was 0.0003% at 0-19 years, 0.003% at 20-29 years, 0.011% at 30-39 years, and 0.035% at 40-49 years. The median for 0-59 year-olds was just 0.035%. These are well within and often lower than the seasonal flu range for the under-60s. The last sentence would be ruled out as disinformation, or misleading, or at the very least missing context.
- In the weekly report for August 14–20, NSW Health said: “The minority of the overall population who have not been vaccinated are significantly overrepresented among patients in hospitals and ICUs with Covid-19” (p. 2). Two pages later, the same report gives us the data for hospital and ICU admissions by vaccination status. The number of unvaccinated is exactly zero for both. Now, this makes it mathematically impossible for the unvaccinated to be “overrepresented” among hospital and ICU Covid patients. There is an important conceptual distinction between the statement on page 2 and the statistics in Table 1 two pages later. The first is part of public messaging by the health department of Covid vaccines being “safe and effective.” The second is actual data. The way I read the amended National Law, and therefore the way that some AHPRA (Australian Health Practitioner Regulation Agency) official could read it at some time in the future against any doctor, the latter must conform to the public message and not mention the actual data.
- Imagine a family of 45-year-old parents with three young children aged 5-12 who visit their family doctor to discuss vaccination for their kids and boosters for themselves, both to protect themselves and their parents in turn as they take the kids to spend quality time with grandparents. In the name of public safety, will Australian doctors have to promote the mRNA vaccines to children, boosters to grown-ups and be forbidden to mention advice to the contrary in Scandinavia and Florida? In New South Wales, of the 2,311 Covid-related deaths since May 22, only 3 have been under 20 and 34 under 50. Has any healthy under-20 died of Covid in Australia through the pandemic? If children are at virtually no risk and vaccines don’t stop transmission, why expose children to the risk of serious adverse events?
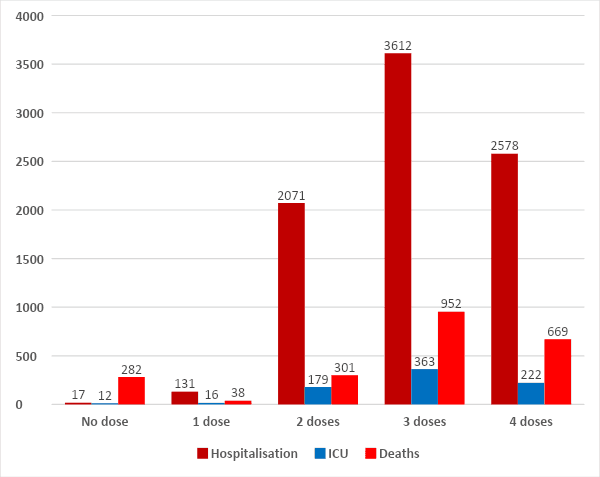
- What of the startling revelation that Pfizer had never tested its vaccines for transmissibility and therefore the entire vaccine passport requirement was built on a conspiracy of lies? In an NBC interview on February 26, 2021 Pfizer CEO Albert Bourla clearly says “there are a lot of indications right now that are telling us that there is a protection against transmission of the disease” provided by the vaccine. In a CBS interview on May, 26, 2021, Anthony Fauci said: “when you get vaccinated, you not only protect your own health, that of the family, but also you contribute to the community health by preventing the spread of the virus throughout the community … you become a dead end to the virus.” Australian data too confirm that while vaccines and boosters continue to provide protective benefits against severe disease and deaths, despite 95 percent adult vaccination they do not provide immunity against infection, hospitalization, ICU admission or even death (Figure 1).
In an article on news.com.au, Frank Chung has done Australians a great service by compiling a list of statements from Australian ministers and health bureaucrats repeatedly stating their firm conviction that vaccines stop transmission. Michael Senger has done us all a service with a similar look back at the demonization of the unvaccinated by various public authorities, only too eagerly amplified by the media, and all predicated in the false belief that vaccines stop transmission.
For readers with an interest in Australia, Richard Kelly provides a review of many head-shaking edicts and enforcement actions – such as fining a delivery man for washing his van at an empty car wash at 1.15 a.m. and a teenage learner driver for going for a lesson with her mum – that were issued by public health officials. Their ignorance about the disease was exceeded only by their arrogance and hubris about their ability to control the behavior of a coronavirus. Would Australian doctors be at risk of deregistration for mentioning any of this?
Oliver May of News UNCUT wrote an open letter to 20 British news editors on October 12, asking them to explain why they had failed to run a story either on the powerful documentary on vaccine injuries called Safe and Effective: A Second Opinion, or on Dr. Aseem Malhotra’s painfully honest peer-reviewed study calling for a pause in Covid vaccination because of serious adverse events until all the raw data has been subjected to fully independent scrutiny. Both would be interesting to the public and both are very much in the public interest. We shouldn’t hold our breath for an answer. Maryland School of Pharmacy’s Peter Doshi, senior editor of the British Medical Journal, is right to call out the legacy media for their lack of balanced coverage of Covid vaccines.
Remarkably, the Pfizer admission has been studiously ignored by the Australian MSM. In case I had missed the coverage of the bombshell interview in the Australian media, I did a search on the website of ABC (Australia’s version of the BBC), Age, Australian and Sydney Morning Herald papers. I got zero hits for Robert Roos, the Dutch MEP who asked the question in the European Parliament of Pfizer director Janine Small, and for the latter who confessed to lack of testing for transmissibility. Fading trust in our principal institutions is contributing to the multipronged global crisis of democracy.
The lack of media interest and coverage means there is little pressure for public accountability. Absent that, there will not be any punishment meted out to ministers and bureaucrats for the extensive range of malfeasance in inflicting cruel and inhumane harms on millions of their citizens; no prospect of emotional closure for the people for the trauma they have suffered, including deaths of despair and desolation born of loneliness; delayed prospects of the masses shedding their sheer dread of a virus that for most healthy people under 70 or 65 is not really a severe illness; and a refusal to institute the most powerful deterrent of all for any repeats of public criminality on a grand scale.
Instead we can all look forward to endless cycles of rinse and repeat of surveillance, compulsion and coercion of the masses on the whims of their technocratic betters.
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








