What is the relationship between education, knowledge, and wisdom? This is not a trivial question, and the ramifications are far from obvious. Our lives may literally depend on it.
Let me illustrate the problem. On 12/5/2025, a Joint Statement from numerous medical organizations was released, highly critical of the recent recommendation of the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention (CDC) on modification of universal administration of the Hepatitis B vaccine to every newborn. The wording of the statement is telling:
“We are deeply alarmed by the actions taken this week by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP). The apparent goal of this meeting was to sow doubt in vaccines rather than advance sound vaccine policy, and we will all pay a price for that.
“This is a significant departure from the historic role ACIP has played in shaping vaccine policy in the United States. Previously, we could expect science to drive decisions, experts to debate evidence, and consensus to lead to shared, clear recommendations. That is not the case with the current committee, and this change puts Americans’ health at risk. (emphasis added)
This is like the statement from the National Foundation for Infectious Diseases from June 27, 2025, regarding the current makeup of the ACIP:
Deviation from the long-standing evidence-based process that has historically guided ACIP deliberations undermines transparency and trust, risks legitimizing misinformation, and is harmful to public health. A process that includes input from Centers for Disease Control and Prevention (CDC) experts, working groups, and trusted scientific and medical organizations, has been critical to ensuring rigorous, transparent, evidence-based recommendations that the public and healthcare professionals can trust. Voting on critical policy recommendations without due process that includes a thorough, balanced, and vetted review of available data by qualified experts invalidates the results and leads to confusion and distrust of recommendations.
On 12/14/2025 Politico published a piece entitled This vaccine adviser to RFK Jr. has some choice words for his critics. It reviewed the firestorm of criticism being leveled at the current members of the ACIP of the CDC as well as the response from Retsef Levi, including:
I think we’ve adopted an extremely medicalized view of health. Our system is very centralized and coercive. Too many public-health policies assume that a small group at the top should make decisions for everyone and enforce them instead of putting the individual at the center and empowering people, with the support of doctors and others, to take ownership of their health.
Some ACIP members and presenters are criticized as not appropriate for the ACIP because they are not physicians or “experts.” My view is quite different, and I agree with Professor Levi. They are terrific choices, not despite not being physician “experts,” but because of it! And I will back this up with clear evidence.
The problem has to do with entrained thinking in both leaders and experts. When both are combined in decision-makers, so is the danger as explained by David Snowden and Mary Boone in A Leaders Framework for Decision Making:
…leaders are susceptible to entrained thinking,a conditioned response that occurs when people are blinded to new ways of thinking by the perspectives they acquired through past experience, training, and success…
Entrained thinking is a danger in complicated contexts, too, but it is the experts (rather than the leaders) who are prone to it, and they tend to dominate the domain. When this problem occurs, innovative suggestions by nonexperts may be overlooked or dismissed, resulting in lost opportunities. The experts have, after all, invested in building their knowledge, and they are unlikely to tolerate controversial ideas. If the context has shifted, however, the leader may need access to those maverick concepts. To get around this issue, a leader must listen to the experts while simultaneously welcoming novel thoughts and solutions from others.
Medicine is a very siloed profession to begin with. We physicians tend to have a great depth of knowledge but may be significantly challenged regarding its breadth. The Dunning-Kruger Effect (lack of knowledge in an area paradoxically causes overconfidence in one’s competence) is noted in medical students, but what about physicians in general?
Surprisingly, I couldn’t find much specific on this, but there are anecdotal reports that would suggest physicians at times make very problematic airplane pilots. Most likely, if true, the reason is complex. However, the “organizational culture” of a physician is most likely at least part of the problem.
In Tribal Leadership, David Logan and co-authors describe 5 levels of Organizational Culture, along with their taglines:
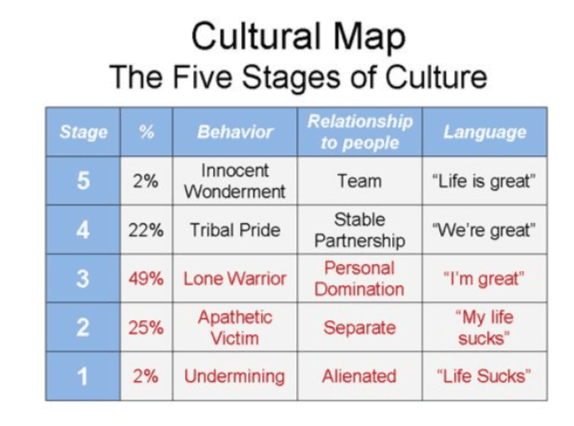
Virtually all physicians are stuck at Stage 3 and acceptance of new ideas can be a difficult undertaking, especially if it involves questioning their authority.
Is there any evidence to support these observations? Are there episodes from history, especially scientific history, to explain this current upheaval with the ACIP? I believe there are:
The Longitude Problem
For centuries marine navigation proved to be difficult if not outright dangerous. While the latitude (North/South position) could be relatively easily ascertained using a sextant, the longitude (East/West) was not. Some of the greatest scientific minds, including Isaac Newton, attempted to solve the problem, but came up empty. In 1714 the Commissioners for the Discovery of the Longitude at Sea established monetary prizes for the most accurate measurements of Longitude, up to £20,000. Many attempted complex celestial trigonometric formulae but it was only when a carpenter and clockmaker, John Harrison, constructed a chronometer that would accurately maintain Greenwich Mean Time aboard a ship that the problem was solved.
Powered Heavier Than Air Flight
Although the claim for the first heavier than air-powered flight is clouded, it is generally accepted that the first flight in 1903 was accomplished by the Wright Brothers, bicycle mechanics and not engineers.
Jet-Powered Aircraft
In 1929, Frank Whittle, a junior flying officer in the RAF, developed the concept of the first jet engine. He used a turbine spun by exhaust gases to run a compressor processing the inflow air. Unfortunately, the “experts” failed to see the genius in the design and had a basic underlying conflict of interest and slow-walked the project. Whittle lacked the academic credentials of those reviewing the project. In addition, the “experts” failed to classify the patent as secret! Hans von Ohain, a trained engineer in Germany working with the support of Ernst Heinkel on a similar idea saw the patent and modified it, allowing the Nazi Luftwaffe to produce the first operational plane.
The “Mother of Wi-Fi”
While most people think of Hedy Lamarr as a beautiful Hollywood actress, she was a genius with multiple inventions including “frequency hopping” that prevented torpedoes from jamming. It also formed the basis for such things all of us use: Wi-Fi, GPS, and Bluetooth. Not bad for an “amateur.”
Polio Rehabilitation
“Sister” Elizabeth Kenny was a self-taught Australian Bush Nurse who broke with the prevailing immobilization of patients with polio and introduced a radical treatment of passive motion. This was not met with enthusiasm by the medical establishment in Australia:
Between 1936 and 1938, a Queensland Government Royal Commission evaluated Kenny’s work and published its Report of The Queensland Royal Commission on Modern Methods for the Treatment of Infantile Paralysis in 1938. Its most critical comment, on Kenny opposing the use of splints and plaster casts was: “The abandonment of immobilization is a grievous error and fraught with grave danger, especially in very young patients who cannot co-operate in re-education.”
Isn’t this response remarkably like the criticism of the ACIP by the current medical establishment in the United States? Interestingly, Kenny’s ideas were received with favor at the Mayo Clinic in the United States.
The Excess Mortality Problem
Numerous authors (Ed Dowd, Debbie Lerman, Denis Rancourt, et al, and others) drew attention to the sudden death of many individuals, including Hank Aaron, in close proximity to injection with the mRNA anti-Covid agents. Most of the early authors, while competent researchers, were not directly involved in medicine or health care. Their findings were criticized by others and this criticism is enthusiastically pushed by organizations such as GAVI. Interestingly, the online comments on this article mention numerous questions regarding the methodology and validity of this study. Other authors, possibly with less conflicts, admit this observation is real and needs further study.
The Flexner Report
Although the subject of criticism because of the current lens of “systemic racism” and “sexism,” there is no doubt that the 1910 report instituted a sea change in both the practice of medicine and medical education. Of interest in the current discussion is what organization conducted the report and the professional background of the author:
In 1908, seeking to advance its reformist agenda and hasten the elimination of schools that failed to meet its standards, the CME contracted with the Carnegie Foundation for the Advancement of Teaching to survey American medical education. Henry Pritchett, president of the Carnegie Foundation and a staunch advocate of medical school reform, chose Abraham Flexner to conduct the survey. Neither a physician, a scientist, nor a medical educator, Flexner held a Bachelor of Arts degree and operated a for-profit school in Louisville, Kentucky.[16] He visited every one of the 155 North American medical schools that were in operation at the time, all of which differed greatly in their curricula, methods of assessment, and requirements for admission and graduation.
Contrast this with the criticism by the numerous medical organizations of the makeup and conduct of the current ACIP that led off this essay. The Flexner Report was NOT conducted by a medical organization and was led NOT by a physician or indeed anybody involved in medicine, but by a B.A. graduate in the Classics, with no advanced degree, who ran a for-profit school in Kentucky!
I do not personally agree with all the conclusions and recommendations of the report. Its emphasis on the scientific method allowed the solution to the pressing “complicated” problems of the time but pushed “complex” problems into the background. It sidelined the influence of the patient and society into the broader question of health care and emphasized disease care.
The Rockefeller Family heavily supported the creation and implementation of the Flexner report. The recommendations fit into the development of pharmaceutical agents and aligned with the interests of the Rockefellers in pharmaceutical agents. This allowed the entry of Big Pharma and set the foundation for the disaster that was our response to Covid.
In a recent essay, David Bell has cogently described the conflicts of interest in the entire governmental health oversight system.
The companies, holding return on investment as their priority, also design and sponsor their own drug trials, and offer senior staff of regulatory agencies like the FDA (whose salaries they already fund through fees paid by Pharma) the prospects of better-paying jobs if they all remain friends. They can sponsor disease modeling to show far higher mortality than real life can provide, and medical journals to publish fairy tales in support of this cause. They sponsor most members of the US Congress for the same reason. None of this is complicated – it is business and nearly everyone understands it…
ACIP was still erring on the side of Pharma, which they presumably have to due to the sponsored-Congress problem. They may have got it right, they may not have. Now the onus is on someone, preferably an independent body like the CDC is supposed to be, to do sensible, well-designed, well-managed, transparent prospective trials in the right populations. It is possible. Only a risk to corporate income and return on shareholder investment could render that idea controversial.
While we may assume that “education” is synonymous with “knowledge,” personal experience reveals that is not necessarily the case! Even putting aside the distinction between “explicit” and “tacit” knowledge, a degree after one’s name is no proof that the subject has been mastered. In a recent blog post, Ankita Singha reviewed the difference between knowledge and wisdom. Even “knowing” the topic (knowledge) may not ensure the correct application of that knowledge (wisdom).
We may in fact be on the cusp of a true Scientific Revolution and Paradigm Shift and need to look at the wisdom of people like Retsef Levi and take his advice to find our way forward:
I think we’ve adopted an extremely medicalized view of health. Our system is very centralized and coercive. Too many public-health policies assume that a small group at the top should make decisions for everyone and enforce them instead of putting the individual at the center and empowering people, with the support of doctors and others, to take ownership of their health.
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








