
Last month, a young student at Eton College died at the age of 17 years while playing games at the College fields. Unfortunately, this sad event is not an isolated incident. During the same week, a different young football player collapsed in 3 separate world football games. As a stunned commentator said, “World football, unfortunately, has been subject to so many distressing scenes on the pitch over the last few years.”
Investigations are urgently needed if we are to cultivate healthy generations by 2040. Trends and observations for children (0-14 years) reviewed in this article confirm that the health of the young population is deteriorating. Unfortunately, until now the sharp decline in children’s immune systems is not capturing the attention of experts and public health authorities.
To rescue children’s health, this needs to be viewed as an emergency. Policies for any poorly investigated drugs or vaccines with serious risks for harmful side effects could be halted until safety and effectiveness are demonstrated through analysis by independent parties.
For a healthy, balanced, and economically flourishing country, the best return on investments will be from programs aiming to support women’s health during pregnancy and children’s health.
Increased Mortality in Children 0-14 Years
The latest numbers on trends in excess mortality on Eurostat, the UK, and the US for children in the age 0-14 years as analyzed by Phinance Technologies can no longer be neglected.
Phinance Technologies estimates excess mortality by computing deathrates relative to a given baseline, rather than by changes in deaths. This significantly improves the accuracy of changes in mortality. The method 2C, as used in figures presented in this article, estimates excess death rates by computing relative to a baseline that is the continuation of a previous trend in excess deaths. The analysis aims to significantly improve accuracy on excess mortality.
Several countries analyzed over the past four years have noticed increases in excess mortality for all ages. Among them are the Netherlands, the US, the UK, and Bulgaria. These are facing a remarkable increase in excess mortality in children 0-14 years in 2021-2023. On the other hand, far less or no excess mortality in children 0-14 years is observed in countries like Sweden, Denmark, and Belgium.
In January 2024 Eurostat Excess mortality statistics reported the highest rates of excess mortality in the Netherlands, followed by Denmark. Ten countries, among them Bulgaria, recorded no excess deaths. Excess mortalities in Eurostat figures are shown in percentage difference versus average monthly deaths 2016-2019 (method 1).
Results on Excess Mortality the Netherlands, the UK, and the US
Data analysis on excess mortalities analyzed by Phinance Technologies are presented in Figures (1-5).
The Netherlands
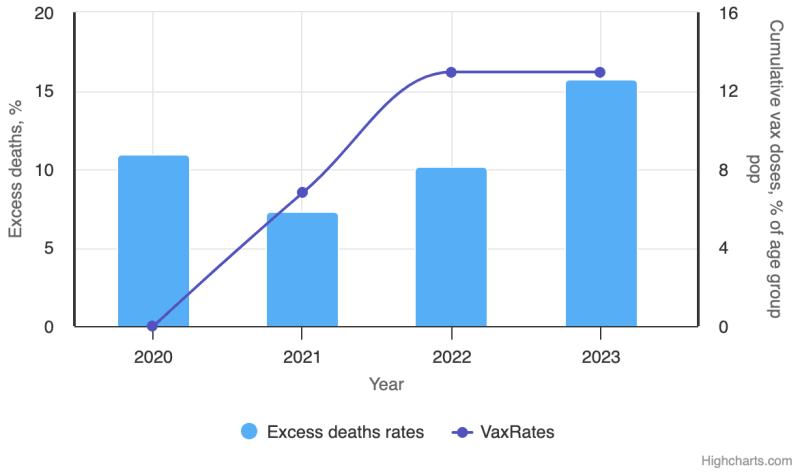
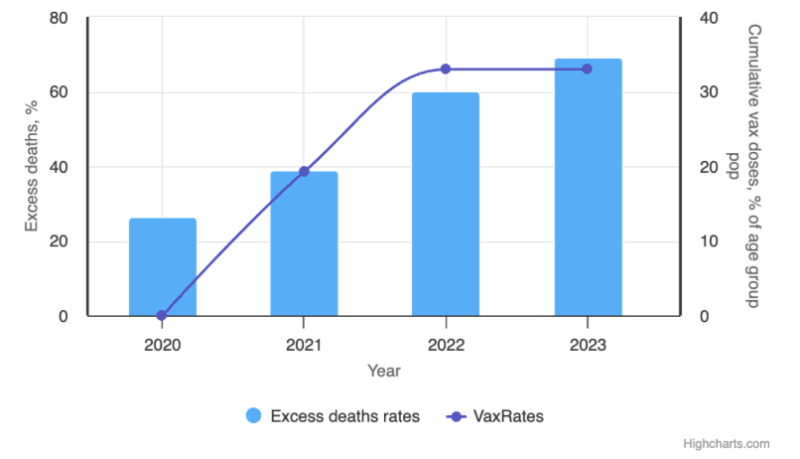
The highest trend in more deaths than expected was found for the youngest age group 0-14 years (Figure 1A).
Figure 1B shows that the Netherlands is facing a public health problem, especially for the age group 10-14 years with a rise in excess deaths more than expected from 2020 onwards, up to a staggering 60% in 2023. In the age group 0-14 years, fewer deaths were observed in 2021 and 2022 than in 2020, but the year 2023 showed 15% more excess deaths than expected (Figure 1A).
Irrespective of the analysis method (1, 2A, or 2C), each used all computing methods of data for the group 10-14 years and showed a trend in more deaths than expected in the years starting in 2020 to 2023.
UK
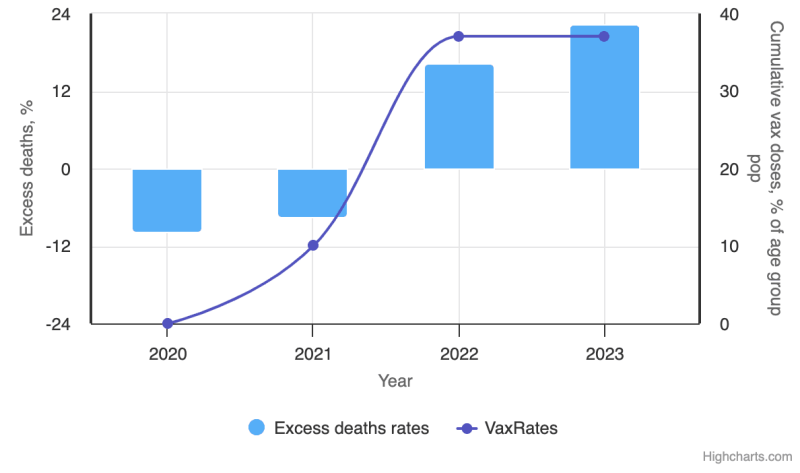
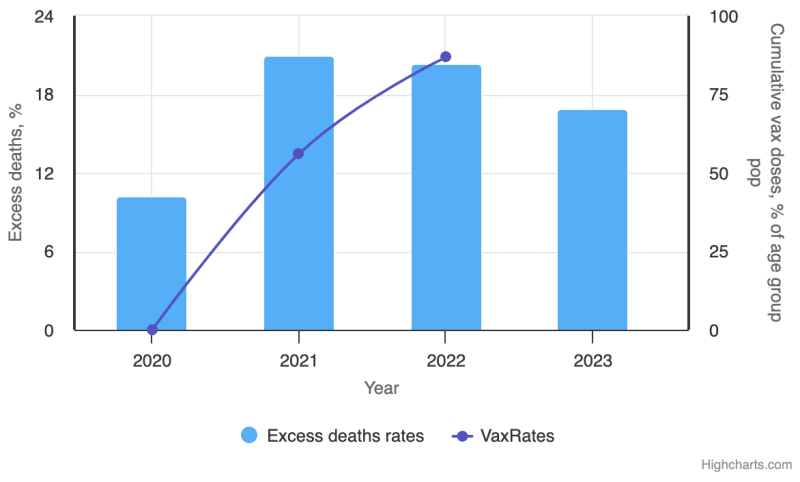
In the UK, excess deaths are up a staggering 22% among 1-14 years old in 2023 (Figure 2A). In 2020, there were 9% fewer deaths. In 2021, there were 7% fewer deaths than expected. In 2022, there were 16% more deaths and in 2023, there were 22% more deaths than expected. Figures from the Office of National Statistics show about 10% more deaths than expected across all age groups.
The UK is the only country reporting an increase in more deaths than expected for newborn babies 0-1 years from 2021 onwards, with 24% more deaths than expected in the year 2023 (Figure 2B).
The highest increase in child death in 2021-2023 was observed in the most deprived quintile of the UK and among black, Asian, and other populations.
USA
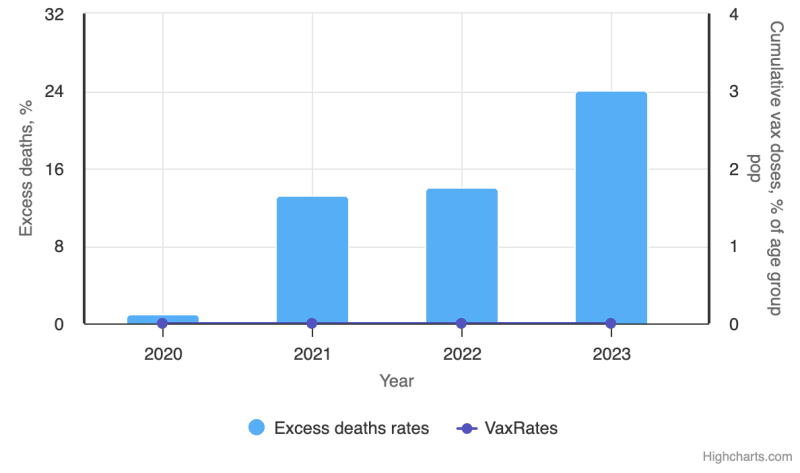
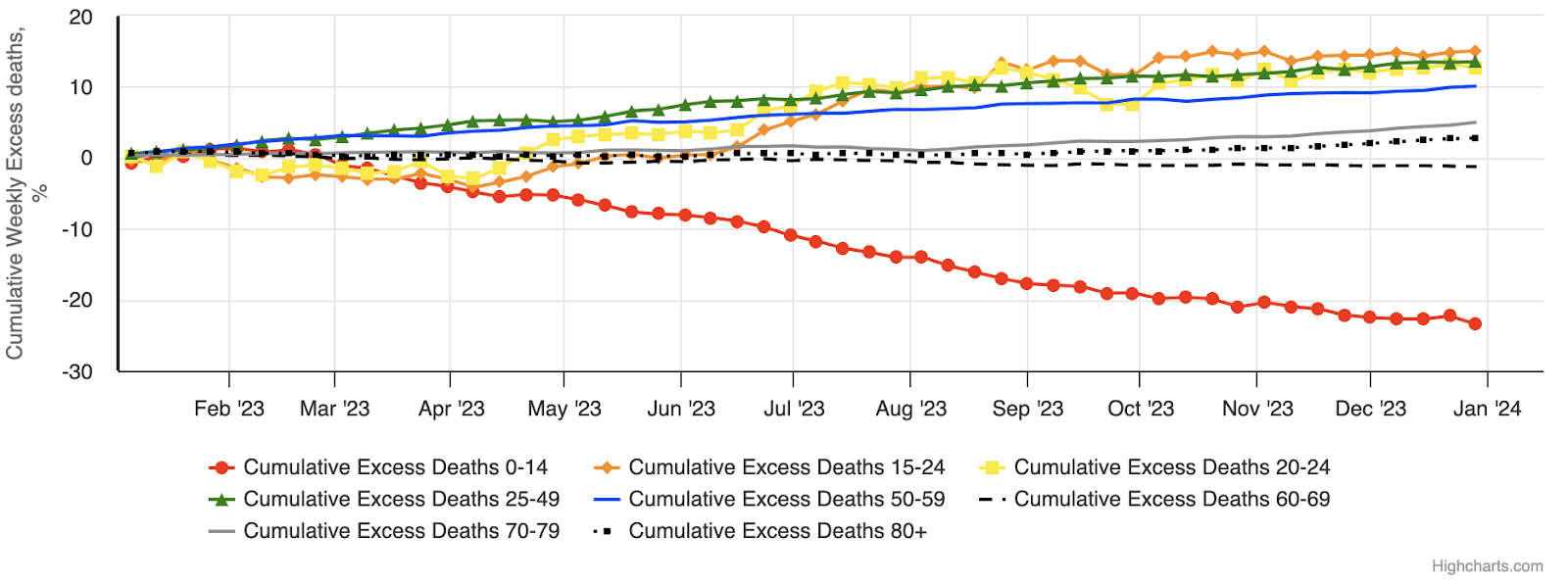
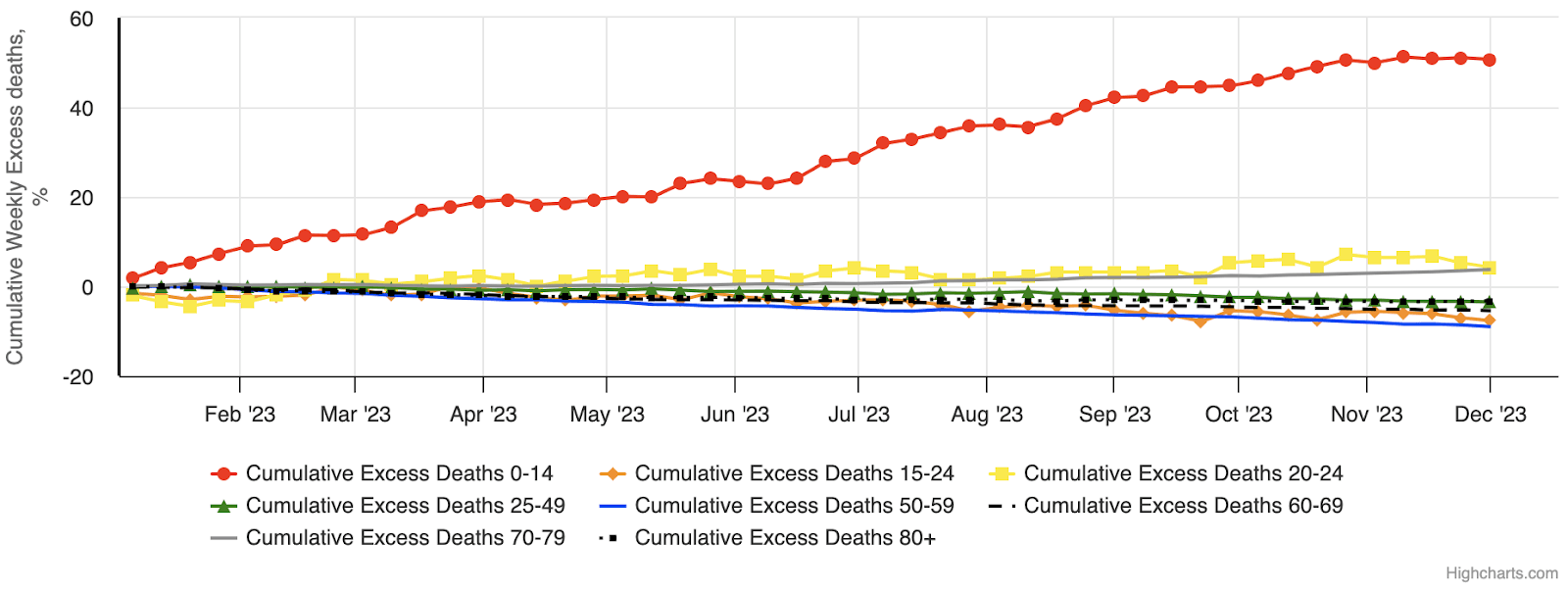
In the US, an increase in more deaths than expected is seen for the age 0-24 years in 2020-2023 (figure 3). As compared to other age groups in 2023, the highest number of more deaths than expected was found for the age group 0-24 years. Unfortunately, specific analysis 2020-2023 for the age 10-14 years is not available for the US.
The VAERS analysis update from 23-2-2024 showed children aged 6 months to 17 years had 192 reported deaths, 90,288 reported injuries, and 11,160 children not recovered from their injuries.
Analysis of VAERS data on all vaccine deaths from 1988-2021 demonstrated that Covid vaccine deaths in one year are equivalent to deaths from all other vaccines.
The recently forced release of hidden CDC data showed that among all age groups, hundreds of thousands of Americans sought medical assistance after a Covid-19 vaccination. The data showed 37,231 reported deaths, 214,906 reported hospitalizations, 1,630,913 adverse event reports. and 2.5 million people reported having to miss schoolwork or other normal activities.
A Mystery
Why some countries observe in children 0-14 years more excess deaths than expected while other countries see fewer deaths than expected is still a mystery.
In 2023, Western ‘rich’ countries with a qualified and expensive healthcare system (the Netherlands) observed more deaths than expected while others (Belgium) reported fewer deaths than expected in children aged 0-14 years (Figure 4).
Bulgaria observes more deaths than expected for children 0-14 years in 2021-2022-2023. The highest increase in more deaths than expected for all age groups was observed in 2021 (data not shown).
In the EU, Bulgaria is a country with the cheapest healthcare system and lowest life expectancy. In the elderly population, there is low Covid-19 vaccine coverage. However, in contrast to all other age groups, the country noticed more children dying than expected in the youngest age 0-14 years (Figure 5).
For children under 18 months of age, vaccinations are mandatory in Bulgaria. Severe Covid-19 infections in the age group 0-14 years are rare. The cause for more deaths than expected is unknown.
The difference among countries in more children dying than expected needs further exploration. From an ethical point of view, it is expected that all countries report all death cases to EU data platforms that are officially used for statistics on excess mortality and comparative analysis between countries. To improve future public health policies, it is highly important that accurate and reliable numbers and methods (estimating changes in mortality) are used for lessons to be learned.
Based on current data, there is a serious warning on the devastating degradation of the children’s immune system. The percentage of immunocompromised children in the worldwide population is rising. In countries with more children dying than expected, public health authorities have a responsibility to urgently investigate possible causes.
More Immunocompromised Children
The biggest public health threat is not a virus but a weakened immune system, as explained in an October 2021 publication. Unfortunately, this is experienced today.
No one can deny that young women and children have been hit hardest during the pandemic.
Over the past four years, women and children have been exposed to more stress, fear, loneliness and anxiety, increased use of medicine (antidepressants, psychotropic medicine, NSAID, antibiotics, immune suppressive, cancer medication), poverty, and vaccinations.
Pregnant women, children, and adolescents are more susceptible to intoxication.
Pregnancy
It is the first time in history that most Western countries recommended three vaccines for pregnant women: mRNA Covid-19 vaccine, DTaP (a combined Diphtheria Tetanus acellular Pertussis) vaccine, and a flu vaccine. In December 2021, the UK prioritized pregnant women for Covid-19 vaccinations or booster injections. A blog at GovUK says it is fine to have the vaccinations at any stage of the pregnancy. The vaccines meet strict safety and effectiveness checks. On March 27th 2024, the Health Advisory Board in the Netherlands decided that a Covid-19 vaccine for pregnant women is no longer recommended.
Long-term effects are not known. Results from clinical trials with lipid nanoparticle and pseudouridine modified mRNA Covid-19 vaccines in pregnant women have long been hidden from the public. Just recently, investigations of the many pages of Pfizer documents released under court, analyzed by Dr. Naomi Wolf and her team, have shown the risks for the harm on the human body and the reproductive system. A research letter published in the American Journal of Obstetrics & Gynecology suggests a transplacental transmission of the Covid-19 mRNA post-vaccination to fetus and baby. Two studies suggest that vaccination during the first trimester of pregnancy produces a greater rate of developmental problems as compared to vaccination during the third trimester. Moreover, mRNA vaccines could have negative effects, increasing the risk of unrelated infections.
Recently, safety concerns put a stop to a maternal RSV vaccine study. They observed 151 more preterm births and 10 more neonatal deaths in the vaccine group. The Health Council in the Netherlands just advised to protect all children against RSV through the national vaccination program. Vaccination of pregnant women is one way to protect the children.
DTaP vaccinations during pregnancy are stated to be safe and effective for the fetus and the mother, as these are not live attenuated vaccines. However, a study with an acellular pertussis vaccination in mice impaired the cellular immunity to Bordetella Pertussis infection in the offspring.
A more than 4,000% increase in miscarriage was found when in 2009-2010 both a pandemic (A-H1N1) and seasonal flu vaccine were administered during pregnancy. A systematic review on the safety of influenza vaccination during pregnancy concluded ‘evidence with very low certainty suggests that seasonal influenza vaccination during pregnancy is not associated with adverse birth outcomes or maternal non-obstetric Severe Adverse Events.’ The low potential benefits (10-60%) of the current flu vaccines have been confirmed in Why flu vaccines so often fail in Science: ‘This immunization program has been predicated on assumptions on top of assumptions.’
Moreover, in the Netherlands 3 out of 4 pregnant women use medicine without knowing if the doses of drugs used during pregnancy need to be different. In April 2024, a platform was introduced for information on the use of medicine during pregnancy. Interactions by medicine and vaccinations on mother, fetus, and baby in the short and long term, as discussed in ‘The collapse of women and work,’ have not been widely studied. A negative interaction of medicine and Covid mRNA vaccines on the human gut microbiome has been found.
Children
An imbalance of the human gut microbiome (gut dysbiosis) is an optimal situation for opportunistic pathogenic bacteria to multiply and a risk to pass a maximum tolerated toxin level into the fetus and child. The damage can vary: infectious disease, invasive bacteremia to chronic diseases, cardiac vascular problems, cancer, early aging, or a sudden death.
Whether or not there has been a confounding of a correlation between the new Covid-19 vaccines and more deaths than expected in children 0-14 years is difficult to assess. Personalized data of the medical history of children would be beneficial to better understand what the ultimate causes of a fatal complication in immunocompromised conditions are.
A recent article from the CDC argues that there is no relation between the vaccine and sudden death in young people. However, a much larger Korean study found 19.8% of severe vaccine-related myocarditis in all vaccine-related myocarditis. The authors concluded that sudden cardiac death should be closely monitored as a potentially fatal complication of the Covid-19 vaccination.
A self-reported physician-diagnosed study in Saudi Arabia found cardiac complications one month to one year post-mRNA vaccination in 27% of individuals who participated. In a Japanese study, increased age-adjusted cancer mortality was observed after a third dose of mRNA lipid nanoparticle vaccine during the Covid-19 pandemic. A population-based study among Danish adolescents of 12-17 years showed that myopericarditis after a Pfizer-BioNTech mRNA Covid vaccination occurred more frequently as compared to US reports.
Unfortunately, in a study with 29 vaccinated children (5-11 years), markedly reduced immune responses were found to pathogenic bacteria like Staphylococcus aureus 28 days after the second doses with Pfizer.
There have been publications that support the recommendation that both children with an underlying medical condition and otherwise healthy children receive an mRNA Covid vaccine. However, there are also publications that conclude that the benefits of the Covid-19 vaccination program for children may not outweigh the risk.
Last week, a leading WHO vaccine expert testified in a lawsuit in Finland. She advised against Covid vaccine passports, as the vaccines did not stop transmission and gave a false sense of security and that this was known in June 2021.
Whereas children 0-14 years had proven long-term and robust natural immunity by early 2021 and it was known that serious infections with SARS-CoV-2 virus are very rare, in numerous countries children were indirectly forced to be vaccinated to participate at schools and sports, travel, or go out.
The introduction of the Covid-19 mRNA vaccine meant one, two, or three extra injections in young children on top of the normal childhood vaccination program. The number of children vaccinated per country varies. Studies on if, when, and how the new vaccines could best be introduced within this standard program were not available or poorly studied.
Moreover, a systematic review on observational childhood vaccination studies has found that the reception of DTP may be associated with an increase in all-cause mortality. Also, a peer-reviewed article on Guinea Bissau found that after the introduction of DTP, there was an increased overall mortality in all studies.
The article, ‘Vaccinology time to change the paradigm?’, an open and transparent reflection on the existing vaccine paradigm, noted that non-live vaccines enhance the susceptibility of girls to unrelated infections.
In the Netherlands and the UK, whooping cough pneumonia has increased far above levels in previous years, especially in the age group 5-14 years. In February-March 2024, 4 babies diagnosed with whooping cough died in the Netherlands. In previous years, this was one to two babies per year.
For children aged 0-4 years, acute otitis media, acute upper respiratory tract infections, jaundice, and gastro-intestinal problems have increased the past two years. Overall, in many countries sickness in children is increasing. It can be whooping cough, hepatitis, adenovirus, MISC, measles, Bird Flu, or disease X. Among the chronic diseases: anxiety, depression, chronic pain, cancer, and diabetes are expected to rise the most.
Unfortunately, as with Covid-19, the data presented on dashboards are mainly filled by data from inaccurate PCR tests. A recent case in court in Portugal decided that results of a PCR test without seeing a doctor are not sufficient for diagnosis.
People with immunocompromising conditions are more vulnerable to a complex infection and inflammation (chronic disease). Though overall patient survival has increased, pneumonia is the most common invasive infection in immunocompromised patients and continues to carry a high mortality and morbidity rate. Possible mechanisms for how opportunistic pathogenic bacteria take over in an impaired immune system is explained via the dramatic degradation of the human immune system.
Vaccinating Immunocompromised Children is Not Without Risk
Immunocompromised individuals may not mount as strong an immune response as healthy individuals. During the pandemic, multiple booster doses have been recommended for immunocompromised individuals and as a result may have become at higher risk for breakthrough infections where they contract Covid-19 despite booster vaccinations.
Recent research has shown that multiple doses of mRNA Covid-19 vaccines may result in higher levels of IgG4 antibodies or impaired activation of CD4+ and CD8+ T-cells. An impaired immune system becomes more vulnerable to infections and inflammation.
Unfortunately, there is a lack of reliable information inferred from long-term studies to evaluate the safety and efficacy of repeated booster doses in risk populations. Even for healthy individuals, repeated vaccinations with the lipid nanoparticle N1 methylpseudouridine mRNA may have resulted in an impaired immune system and a higher risk for cancer or infectious diseases.
Overall long-term effects of childhood vaccination programs in immunocompromised malnourished children have been poorly studied. Even in the absence of infection, malnutrition is generally a pro-inflammatory disease.
Since the introduction of the acellular Pertussis vaccine, it is well known that despite widespread vaccine coverage, the number of cases of pertussis reported in high income countries has increased, with a characteristic peak every 2-5 years.
It is worth reflecting on the statement that Pertussis is rising due to declining vaccine coverage. Impaired immune systems have been observed after the third through fifth injection with DTaP vaccine.
Moreover, many studies have shown that the acellular subunit Pertussis vaccine does not stop transmission. Vaccinated children or immunized healthy adults can carry high numbers of Bordetella Pertussis colonies. Still, experts and politicians are arguing for compulsory DTaP vaccination to prevent transmission. Vaccination ad campaigns to boost childhood immunizations are back.
Countries may use DTaP vaccines with different formulations, detoxification methods, and doses, and they may differ in schemes for the childhood immunization programs which may influence immunogenicity and side effects. For example, a detoxified Pertussis Toxin vaccine has been used for more than fifteen years by Denmark and Sweden in preventing whooping cough, resulting in low child mortality. Both countries were cautious early in the pandemic to vaccinate healthy children with Covid-19 mRNA vaccines and have low to no excess deaths in the young age group.
The sequence of injections of various vaccines or vaccines given on one day may have a different influence on healthy children as compared to children with a medical condition. Local and demographic factors may influence safety and efficacy patterns, as well as decision-making and nuanced understanding of how the interventions influence the body’s homeostasis.
A risk for an impaired immune system and a gut dysbiosis is the exacerbation of toxin producing opportunistic pathogenic bacteria like Bordetella Pertussis and Streptococcus pneumoniae. Especially babies are at the highest risk for serious disease and sudden death.
Several pathogenic viruses, including adenovirus, rhinovirus, and influenza have been detected in the airways of patients and infants with confirmed pertussis. Pertussis toxin may suppress the early innate host response needed to control virus infection. Intact and balanced gut microbiota inhibits the colonization of Bordetella Pertussis in the lungs.
There is much to be learned from a traditional way of life with fewer chemical therapeutic interventions. Amish children seem to be less vulnerable to infections and allergies.
Better strategies or therapeutics need to be developed to alleviate diseases in children.
Stop the Mania, Let the Children Play
Without a change in policy, a decline in skyrocketing sickness in the children 0-14 years and a turn to fewer deaths are not expected.
It is time for reflection for anyone following or spreading news outlets and advertisements, or else we will suffer another mania and era of politicised science driven by the same mistakes that already dramatically harmed us.
Japan has learned and has turned to saving children’s health, protecting bodily autonomy, and establishing a flourishing economy.
The strategy of forever adding chemical interventions is not without risks. It is not always known if a child is immunocompromised with the risk for a wrong intervention at the wrong time that could develop into a severe disease or become fatal. Nuances, dialogue, and shared decision-making may be a way to restore trust.
The choice for humanity is to support pregnant women and children with affordable, high-quality, traditional, and nutritious food and let children play.
Join the conversation:
[Sassy_Follow_Icons social_networks="x=https://x.com/brownstoneinst,facebook=https://www.facebook.com/brownstoneinst,telegram=https://t.me/brownstoneinst, truth_social=https://truthsocial.com/@brownstoneinst, linkedin=https://www.linkedin.com/company/brownstone-institute/, gettr=https://gettr.com/user/brownstoneinst, gab=https://gab.com/brownstoneinst" shape="round" style="background-color:#ac3900;]
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








