
On 25 May 2025, after three years of negotiation under the auspices of the World Health Organization (WHO), the Pandemic Agreement was adopted. In reality, the vote was a provisional outcome of an incomplete treaty which postponed decisions on a number of contentious articles, including the required financing, sharing of intellectual property and biological samples, and transfer of manufacturing know-how and pharmaceutical products on concessional terms, to follow-up negotiations.
The objective of the treaty ‘is to prevent, prepare for and respond to pandemics’ and, to this end, its provisions will ‘apply both during and between pandemics.’
Parties also committed to developing a Pathogen Access and Benefit Sharing System (PABS), in the form of an annex to the pandemic treaty, through negotiations in order to promote rapid and timely sharing of materials and sequence information on pathogens with pandemic potential. In return, as part of benefit sharing, participating manufacturers would commit to donating a percentage of their real-time production of safe, high-quality, and effective vaccines, therapeutics, and diagnostics for the pathogen causing the pandemic emergency. An additional share of the products would also be made available to the WHO ‘at affordable prices.’
The treaty cannot be opened for signature until after the PABS has been negotiated and adopted. It will enter into force 30 days after 60 countries have ratified the treaty. A party may withdraw from the treaty at any time after two years from membership by giving a one-year notice.
The beleaguered WHO hosted a total of six rounds of oftentimes acrimonious negotiations on the plan to run the global infrastructure for future pandemics. The original timeline had set a negotiated PABS to be adopted by the World Health Assembly, the governing body of the WHO, at its annual session in May this year. Instead, on 1 May the WHO conceded that even the resumed sixth session of the Intergovernmental Working Group (IGWG) on the WHO Pandemic Agreement had failed to bridge the differences. Accordingly, the Health Assembly will be asked to extend the mandate of the IGWG so it can present an agreed PABS system for adoption in May 2027. The next IGWG negotiating session is scheduled for 6–17 July.
The Risk of Institutionalising WHO Governance Deficits
The text currently under negotiation risks institutionalising the governance failures that defined the Covid-19 response rather than correcting them. It concentrates authority in the WHO without adequate accountability to member states, locks in emergency-mode assumptions about future health, and risks overriding the sovereign responsibility of national governments to determine health policy for their own populations. It would entrench existing inequities while burdening developing countries with unrealistic financial and compliance demands. It is therefore a bad deal for low- and middle-income countries, which make up the majority of the world’s population.
To be clear, the talks are not failing because countries disagree—that is to be expected in any serious negotiation. They are failing because dissent on the parameters of a contested framework is being managed and deflected, rather than engaged and accommodated. The process appears designed to produce agreement using the language of creative ambiguity. When an agreement becomes a proxy for institutional success that masks substantive disagreement over purpose and pathways, the goal has shifted from ‘getting it right’ to simply ‘getting it done.’
Rather than prompting a fundamental rethink, these concerns are being absorbed into incremental adjustments—tweaks to language, minor concessions on access or vague commitments to future flexibility. The concerns raised by Global South delegations reflect real structural tensions in the global health system between public and private goods, donors and recipients, and centralised control and national sovereignty. These cannot be resolved through procedural compromise alone.
The North-South Divide on the WHO Pandemic Agreement
In my major book on the United Nations (Cambridge University Press, 2006 and 2017), I identified the North-South divide as one of the major undercurrents running through the world’s peak international organisation. I built on that work for a briefing paper for Friedrich Ebert Stiftung in 2008, Towards a Less Imperfect State of the World: The Gulf between North and South. That divide remains an important dimension of the politics of the UN system.
As reported among others by Kerry Cullinan for Health Policy Watch on 23, 25, 30 March, and 5 May, ‘final’ negotiations over it were contentious and failed to arrive at a consensus. The split is largely along the global North-South divide. Between them, the Africa Group and the Group for Equity represent the vast majority of WHO member states. They are reported to ‘have become increasingly frustrated’ by the developed countries acting to protect the interests of their pharmaceutical companies instead of agreeing to an equitable sharing of obligations and benefits. Speaking for both groups, South Africa noted that member states were ‘still far from reaching consensus on the text of the Pandemic Agreement annex’ and expressed ‘deep regret’ at the unsatisfactory outcome.
One the one side, the WHO is facing huge pressure from developed countries. The US has cut all funding and Germany has slashed support as well. A quarter of the WHO’s staff are being let go. This has left the WHO ever more reliant on its three biggest donors—Bill Gates (16.8 percent), the vaccine alliance GAVI (which itself gets substantial Gates Foundation funding) and the EU.
On the other side, many developing countries argue that the proposed deal is the latest example of the WHO’s agenda having been captured by Western pharmaceutical companies which take funding from more critical current needs like fighting malaria and TB. They bridle at a power structure perceived to be neocolonial.
Afro-Asian countries are not rejecting cooperation. They are questioning whether the proposed text will deliver equitable outcomes. It risks creating a system in which the costs of preparedness are socialised but benefits are part-privatised. Countries are obligated to share pathogen data—effectively contributing to a global public good. That data will then be used within a complex architecture of advance purchase agreements, manufacturing guarantees, and research incentives that largely benefit a small number of pharmaceutical firms and the Global North countries in which they are based. Many lower- and middle-income countries see a system in which they are asked to contribute data, commit funds, and accept binding rules—while receiving only legally uncertain access to the resulting products, often at negotiated discounts that remain contingent and limited.
To digress briefly but not irrelevantly, many countries in the Global South have muscle memory of the unequal nonproliferation-disarmament obligations of the 1968 Nuclear Nonproliferation Treaty (NPT). Non-nuclear weapon states accepted binding and specific obligations not to acquire the bomb and to adopt IAEA-supervised safeguards to ensure peaceful uses of nuclear power (Articles 2, 3). In return, the five nuclear-weapon states (US, USSR/Russia, UK, France, China) committed ‘to pursue negotiations in good faith on effective measures relating to cessation of the nuclear arms race at an early date and to nuclear disarmament’ (Article 6).
In other words, the disarmament obligation was aspirational, vague, and open-ended and, 58 years later, is yet to be honoured. The same five countries are also the five permanent members (P5) of the UN Security Council and rigorous in efforts to enforce the nonproliferation obligations through their P5 status. The majority of NPT states parties got so frustrated that in 2017 they adopted the nuclear ban treaty against the united opposition of the P5 by a vote in the UN General Assembly.
As the Americans say, fool me once, shame on you. Fool me twice, shame on me.
During the most recent but inconclusive sixth negotiating session in March and April, reflecting the views of many delegations, Pakistan insisted that an agreement should not be rushed simply to ‘manufacture a multilateral success.’ Indonesia, speaking on behalf of the regionally diverse Group for Equity, said that ‘some of the sticky issues are not about time but the willingness to find meaningful solutions. The time pressure alone should not lead us toward weak design, diluted commitments, or lowered expectations.’ When an agreement becomes a proxy for institutional success that masks substantive disagreement over purpose and pathways, the goal has shifted from ‘getting it right’ to simply ‘getting it done.’
At the same time, there is growing recognition that sovereignty comes with responsibility. At a conference hosted by the Economic Commission for Africa (ECA) in March, Clever Gatete, Executive Secretary of ECA observed that health sovereignty is part of national sovereignty. African Ministers and corporate leaders said that Africa must end reliance on foreign aid because ‘health security cannot be mortgaged to foreign funding.’
Similarly, the G20 leaders’ summit in South Africa in November had called for a move beyond traditional aid structures to build resilient, sovereign health systems across the Global South. On 3 April, the Accra Reset Chancery announced that an 18-member high-level panel had been formed to make recommendations on reforms in global health architecture and governance in order to strengthen equity and sovereignty for countries in the Global South.
As it happens, much of the heavy lifting has been done over the past 18 months by a ten-member panel of the International Reform Health Project (IHRP). The project has recently published two reports under the title The Right to Health Sovereignty. The Technical Report provides the analytical foundation, examining ethics, institutional history, disease burden, financing, governance structures, and legal frameworks. The Policy Report distils these findings into principles and reform pathways for policymakers.
Regionalised Burdens-Benefits Equation of Disease and Medical Interventions
The IHRP identifies several interrelated trends, including expansion beyond core public health functions (mission creep and drift), as well as centralisation of authority justified by emergency framing and growing dependence on earmarked and nonstate donor funding. These developments have not merely reduced efficiency; they have eroded trust and legitimacy. To restore faith and confidence, there is urgent need to affirm the notion of health sovereignty and the long-held traditional medical principles of beneficence, non-maleficence, patient confidentiality, and informed consent.
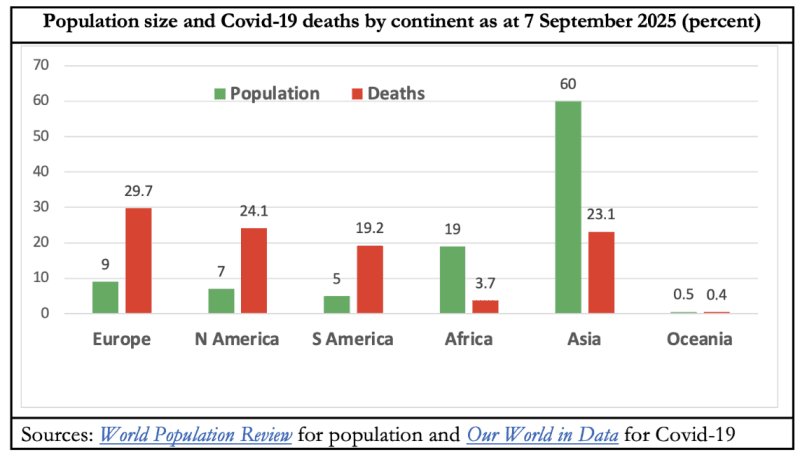
One of the most consequential flaws of WHO-centric global health governance highlighted by Covid-19 was how sharply different were the impacts of the disease across the world. Ditto the policy interventions in response.
The Policy Report documents the strikingly regional Covid mortality toll. Europe and the Americas experienced three to four times more Covid deaths than their population shares while Asia and Africa were three to five times under-represented. According to officially reported data, Covid-19 was the second biggest killer of Americans and the third biggest of the people of the United Kingdom in the four years 2020–23 inclusive. It fell outside the top ten for Egypt, India, Japan, and Singapore. It did not even make it to the top 25 killer diseases reported for the likes of China and Nigeria.
On the other side of the equation, there was an abundance of early warnings, from established, credible, and reputable bodies, on the range of grave harms that were likely to result from population-wide severe lockdown measures. There were impassioned attacks on the immoral and callous indifference of epidemiologists to the deadly consequences of their prescriptions for millions of lives and livelihoods around the world.
The BBC reported on 25 March 2020—that is, pretty much at the start of the Covid-19 pandemic—that ‘India’s poorest’ people ‘fear hunger may kill us before coronavirus.’ In January 2022, Unicef reported on the devastating setbacks to children’s education. Robert Jenkins, Unicef Chief of Education, said ‘we are looking at a nearly insurmountable scale of loss to children’s schooling.’
I argued early on that the biggest tragedy would be across the developing world, with tens and hundreds of millions more people pushed into extreme poverty, additional dead from increased infant and maternal mortality, hunger and starvation with more poverty and disrupted crop production and food distribution networks, sharp cutbacks in children’s immunisation and schooling, destruction of the informal sectors of the economy in which daily wage earners earn a pitiful living, and an upsurge in child labour and trafficking.
Lockdowns, which until 2020 the WHO had explicitly rejected for dealing with pandemics, forced 500 million children around the world out of school, half of them in India. Dr Sunita Narain, Director General of the Centre for Science and Environment, said in February 2021 that more than half the world’s additional 115 million people were pushed back into extreme poverty live in South Asia. India, she said, was all set to usher in a 375 million-strong ‘pandemic generation’ of children up to age 14 who are likely to suffer long-lasting impacts like increased child mortality, being underweight and stunted, and educational and work-productivity reversals.
Little wonder that in a sombre national address on 20 April 2021 shorn of his usual bombast and bravado, PM Narendra Modi ‘urged the states to…work together to save the country from lockdown’ (emphasis added).
Unicef’s State of the World’s Children 2023 report came to the alarming conclusion that ‘in just three years, the world has lost more than a decade of progress.’ Vaccination coverage had decreased in 112 countries and 67 million children had missed out on at least one vaccination over 2020–23 because of lockdowns-caused disruptions and diminished confidence in vaccines. Overall, Unicef recorded ‘the largest sustained backslide in childhood immunisation in 30 years.’ To compound the misery of rising vaccination hesitancy, the WHO reported that vaccination rates against measles fell in Europe and the UK with a 45-fold annual rise in measles cases in 2023. Polio cases were also up by 16 percent.
While some of this might be the lingering effect of lockdown-era disruptions of immunisation services, in part it also arose from falling trust in public health edicts and institutions that spilled over into more generalised vaccine hesitancy. Out of 55 countries that Unicef looked at, public perceptions of the importance of childhood vaccines fell in 52 countries, by as much as 44 percent in some cases. China, India, and Mexico were the only countries where faith in vaccines held firm. The report warned that ‘the confluence of several factors suggest the threat of vaccine hesitancy may be growing,’ including ‘uncertainty about the response to the pandemic…declining trust in expertise, and political polarisation.’
Subsidiarity
Sovereignty is the foundational principle of world order and of the entire multilateral order with the United Nations at the centre. ‘Subsidiarity’ is the principle that policy decisions are taken at the lowest possible level and closest to where they will have their effects.
In the five-year period from January 2020–25 in which 7.1 million people died with Covid, about 203.5 million people would have died from non-communicable diseases and another 38.5 million from non-Covid infectious diseases. (It’s worth emphasising that the Covid death toll refers to deaths with Covid. Deaths from Covid would have been considerably fewer.) In India, Covid-related deaths in the three years 2020–22 (the deadliest years for Covid) were fewer than deaths, in order, from heart diseases, lung disease, stroke, flu and pneumonia, cancers, TB, diarrhoea, diabetes, and even traffic accidents—and almost the same as from deaths by suicide, in many of which the Covid policy harms would have been a contributory factor.
As already noted, the balance of Covid risks and policy-intervention benefits varied between rich and poor countries and between those with good public health infrastructure (for which economic prosperity is a key enabling condition) and those without. Therefore authorities have to work out the best mix of mitigation measures for their own jurisdiction and not fall into the trap of ‘What’s good for Europe is good for Africa’ approach.
This is why the primary responsibility for people’s health should always remain with the countries directly. Regional organisations like the Southern African Development Community (SADC) and the Association of Southeast Asian Nations (ASEAN) should have secondary responsibility for coordinating health policies and initiatives within their jurisdictions. And global institutions like the WHO should be restricted to providing normative guidance, technical support and certification, and data.
International Cooperation
The last remains important because international cooperation in health is necessary and valuable. Cross-border surveillance, data sharing, and technical assistance have contributed to dramatic gains in life expectancy, particularly in developing countries. But multilateral cooperation derives legitimacy from voluntary state participation. When authority drifts towards centralised technocratic bodies detached from domestic accountability, legitimacy weakens—even if intentions are benign.
Accordingly, the goal of reforming global health is not institutional destruction, but restoration of legitimacy through clarity of purpose and accountability. The Policy Report advances a conception of health sovereignty of individuals and countries that is grounded in responsibility, not isolationism. People bear primary responsibility for ensuring their individual health and states for protecting their populations’ health. International organisations exist to support states—not to replace or override them.
The IHRP reports elucidate principles for reforming the WHO—or, if necessary, establishing a successor International Health Organisation (IHO). The IHO must be given limited and clearly defined mandates, with success measured by contraction and redundancy, not expansion of mandates and growth of authority, personnel, and resources. The report pays particular attention to decentralised authority. Emergency powers must be proportionate to demonstrated, evidence-based risk and the highly-differentiated disease burden in the Global South compared to the global North.
The reports aim to promote cooperation, coordinated response, science-based decision-making, and a return to foundational determinants of health over pharmaceutical and technological interventions. Effective cooperation requires legitimacy—and legitimacy requires ethics, evidence, proportionality, respect for the sovereign responsibility of individuals and states, and subsidiarity as the organising principle of the architecture of national, regional, and global health governance.
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








