
On about the 1st of December 2021, the world will pass a notable milestone: more doses of Covid-19 vaccines will have been administered than there are people in the world. The two ‘clocks’ that let me predict this date are here and here. Of course, some people have had three (or more) doses, and others none but already a majority of the world’s population have been jabbed at least once with a Covid-19 vaccine.
Given this massive rollout, we should start to see some effects in the aggregate data. Such data provides observational evidence—correlations rather than causal relationships. Yet these correlations can be informative, especially as pivotal randomized control trials for Covid-19 vaccines, that might be expected to reveal causal effects, were not designed to answer the questions many people have about the vaccines.
Here is what the chief medical officer at Moderna told the BMJ in 2020 about whether the trials tested for protection against infection—what we normally think of with a vaccine:
“…Our trial will not demonstrate prevention of transmission…because in order to do that you have to swab people twice a week for very long periods and that becomes operationally untenable.” (Tal Zaks, chief medical officer Moderna).
Likewise, the trials were not designed to find out (nor did they find out) if the vaccines protected against deaths and hospitalizations. Those events were too rare for the trials to have any statistical power over those outcomes. Here again is what the chief medical officer of Moderna told the BMJ:
“…Would I like to know that this prevents mortality? Sure, because I believe it does. I just don’t think it is feasible within the timeframe [of the trial]—too many people would die waiting for the results before we ever knew that.” (Tal Zaks, chief medical officer Moderna).
Even the pivotal trial for the Pfizer vaccine, with about one-third larger sample than the Moderna trial, had too few deaths to draw firm conclusions. For what it is worth, there were more total deaths in the vaccinated group than the placebo group. In other words, a universe where everyone is vaccinated has more people dying than in a parallel universe where no one is jabbed but otherwise they had the same pre-jab attributes, on average, as the first universe.
It was therefore disingenuous, dishonest even, for health bureaucrats Walensky, Walke, and Fauci to write a “Viewpoint” in JAMA in February 2021 that claimed:
“…Clinical trials have shown that the vaccines authorized for use in the US are highly effective against COVID-19 infection, severe illness, and death.”
Quite rightly, Dr Peter Doshi, a BMJ editor and expert on critiquing clinical trials, wrote a comment showing the claim is false. Yet as Jonathan Swift said 300 years ago, “falsehood flies, and the truth comes limping after it.” So months later, halfway around the world, the largest newspaper in my country had the following about the vaccination status of Green Bay Packers quarterback Aaron Rodgers (who knew New Zealand had so many cheeseheads?)
“…The Covid-19 vaccines authorised for use in the US were tested in tens of thousands of people and proven to be both safe and effective at dramatically reducing the risk of serious disease and death.”
Of course this claim, along with many others purportedly based on the trials, is untrue. Given that the clinical trials have been so prone to misinterpretation, and that they were unblinded early, meaning that efficacy beyond six months cannot be established from the trial data, we have to look elsewhere for evidence.
Several recent studies have used data from nationwide registries or from healthcare providers, to statistically match vaccinated and unvaccinated people to see how fast vaccine efficacy wanes—it falls fast, by about 10 percentage points per month for protection against infection while confidence intervals on severe outcomes like death are often so wide that by six months after the second dose zero efficacy cannot be ruled out.
These are clever studies and it is amazing the data held about individuals that researchers can access. Nevertheless, these studies assume ‘selection is on observables’ which may be a poor assumption for the personal choice of whether to get jabbed. With selection on observables the only things determining if someone is jabbed or not are attributes that the researchers can see in the database.
Instead if unobservable factors—risk preferences, personal beliefs, and so on—affect vaccination choices and also affect health outcomes, the empirical comparisons between vaccinated and unvaccinated may give biased estimates of effects of the vaccine. This is why randomized trials are used; the treated group and the placebo group should, on average, have the same pre-treatment characteristics (both observed and unobserved).
The aggregate data do not solve this selection problem but because all of the evidence is so impure—badly designed and misinterpreted randomized trials, individual level studies that rely on matching self-selected vaccinees against unvaccinated individuals without concern for potential biases coming from unobservables—we should look in all places for insight. Also, the aggregate data are right under our noses due to the proliferation of various websites that provide up-to-date country level (and even sub-national) health and economic data.
The analysis of aggregate data is right in the wheelhouse of economics. Yet economists have been surprisingly absent from public discussions during the pandemic. It is unclear how much of this invisibility is due to the supply-side versus the demand-side. On the supply-side, Jay Bhattacharya suggests in an interview that there was a failure by the discipline to speak up about costs of lockdowns, and to document their collateral damage. On the demand-side, former Governor of the central bank of New Zealand (and then, subsequently, Parliamentary Opposition Leader) Don Brash notes that politicians took Covid-19 advice from some pretty unlikely sources while neglecting input from economists.
Irrespective of reasons for this prior invisibility, economists are now starting to emerge from their cocoons and their analyses of the aggregate data are becoming available. In terms of the global vaccine rollout, it seems that economic conditions matter more than health conditions. Across 112 countries, the rollout was faster for richer not sicker countries. Amongst OECD countries, which have timely and reliable mortality data and are highly vaccinated, rollout was faster for countries where the negative economic shock in 2020 had been bigger, but not where the health shock (excess mortality) had been bigger.
Evidence is also emerging on aggregate effects (and non-effects) from mass vaccination. For 68 countries with full data available, a simple scatter plot shows there was no relationship between the percentage of the population fully vaccinated (by early September, 2021) and new Covid-19 cases in the last 7 days. A concern with such cross-sectional studies is that omitted factors drive the correlations.
For example, my home is a remote country in the South Pacific, whose huge moat was supplemented by strict border controls and almost complete collapse of inward air travel, allowing both low vaccination rates for much of 2021 and low Covid case numbers. Remoteness accounted for both numbers. Another example is when infection rates rise seasonally due to weather that drives people indoors; a country might then ramp up the vaccination effort, given the desire of politicians to be seen to do something whenever a bad thing happens, but it is the seasonal change that is the driving force.
A standard economics approach to these issues is to use panel data (repeated observations on the same countries). With such data we can remove the effect of (time-invariant) unobserved characteristics of countries and (spatially-invariant) unobserved features of time periods to mitigate the impact of omitted factors in driving correlations.
Such panel data for 32 highly vaccinated OECD countries (over 1.3 billion doses to date) that also have high frequency all-cause mortality data indicate that aggregate effects of mass vaccination are showing up in the political-economy sphere but not in health terms. The chart below shows relationships between the fully-vaccinated rate and two health outcomes (deaths from Covid-19 and from all-causes), three economic outcomes (personal mobility to various types of places tracked by Google), and one policy outcome (stringency of lockdown rules).
The outcomes are the change from the same month of 2020, when vaccines were unavailable, versus 2021, when mass vaccination was underway (for each month to September). The units for the chart are standard deviations, to allow comparisons across outcomes in various native units (an index for lockdowns, percentage changes for mobility, rates for deaths).
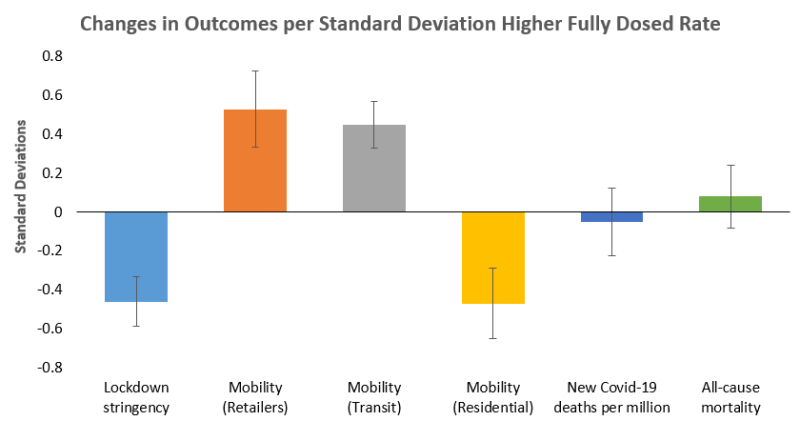
A standard deviation higher fully vaccinated rate is associated with lockdown stringency of one-half a standard deviation lower. This reflects politicians of all stripes tying lockdown to vaccination rates. For example, in September 2021 the New Zealand Prime Minister said “We’re in lockdown because we do not have enough New Zealanders currently vaccinated…” Earlier in the year, UK Prime Minister Boris Johnson said “The way to ensure this [lockdown easing] happens is to get that jab when your turn comes, so let’s get the jab done.”
The rebound in economic activity, as measured by change in consumer mobility compared to the same month of 2020 (so accounting for seasonal factors) is more than one-half a standard deviation higher per standard deviation of the fully vaccinated rate, for retail and recreational locations (and almost as large for transit stations). Conversely, time spent in residential places is about one-half a standard deviation lower, compared to the same month of 2020, in months or countries where the fully vaccinated rate is one standard deviation higher.
Is this rise in being out-and-about due to the vaccines per se, perhaps by making people feel safer, or is it just the response to relaxed lockdown controls? It turns out that it is just the relaxation in lockdown stringency that drives the rise in consumer mobility. Once this is accounted for, there is no independent effect of the vaccination rate on the Google Mobility indicators. So we can think of the jabs as being a jab in the arm of politicians to relax their iron grip on the freedom of movement for people.
While the correlations for mobility (as an economic activity proxy) and lockdown stringency are large and precisely estimated, the corresponding effects on aggregate health indicators are not apparent. Specifically, for these countries through September 2021, vaccination rates have no relationship with changes in new Covid-19 deaths per million, nor with changes in all-cause mortality. After 1.3 billion doses for these countries (and seven billion doses worldwide), one would expect to see some reduction in deaths. Yet such an effect does not show up in these data.
From these results it seems that mass vaccination is some sort of get-out-of-jail card, as a way to get out of ruinously expensive lockdowns and allow some rebound in economic activity. Yet it was politicians and health bureaucrats who put us in jail in the first place. At any time they could undo what they imposed, with or without mass vaccination. As lockdowns failed to control the virus, and did not reduce excess mortality, politicians could have undone these costly and ineffective interventions without needing to rely on mass vaccination.
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








