Last academic year saw most colleges and universities impose some sort of requirement for students, faculty and staff to take the COVID-19 vaccine. While some universities allowed exemptions for religious and/or medical reasons, some did not.
Now a new academic year is around the corner, and things have changed slightly. Some universities have dropped their mandates, others have become more equitable in allowing religious and/or medical exemptions in light of lawsuits either they have faced or neighboring institutions have faced, and still others are still mandating the vaccine, requiring students, faculty and staff to renew exemptions if they had them.
While the scientific justification and ethical basis behind these mandates was questionable last year, with an additional year of research, mandates are even more controversial. Here I present the latest objections to these mandates.
Mandates are not scientifically justified
Scientific studies, reports by health agencies, and other public data have generally shown that vaccination does not prevent infection, thereby not preventing transmission.
Multiple studies (published by the CDC, researchers at the University of Wisconsin, and researchers at Oxford in the UK) have shown that viral loads and/or infection rates are similar in vaccinated and vaccinated individuals. This is important because it is generally understood in infectious disease epidemiology that transmission probability is highest in individuals with the highest viral loads. Another study showed that the Delta variant can transmit easily from vaccinated people to their household contacts, and that the peak viral load in vaccinated remained similar to the unvaccinated.
Even the WHO warned that “There is now consistent evidence that Omicron is spreading significantly faster than the Delta variant” and “And it is more likely people vaccinated or recovered from COVID-19 could be infected or re-infected”. They further suggested that the omicron variant of COVID-19 is “markedly resistant” to the current COVID-19 vaccines, antibody treatments and COVID-19 vaccine booster shots.
A recent tweet by Dr. Vinay Prasad illustrates the vaccine’s decreased effectiveness over time, especially in response to specific variants of the virus. Here is the figure from that tweet, showing how vaccine effectiveness plummeted once the omicron variant became the predominant variant.
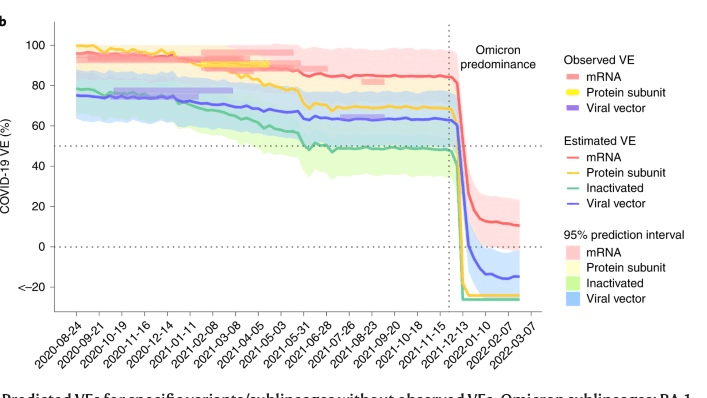
This is consistent with several reports in the media, multiple scientific studies, and multiple op-eds by doctors showing waning effectiveness of the vaccine and high case numbers in population groups with high vaccine coverage.
Moreover, studies from the Cleveland Clinic, researchers in Israel, and another study out of Israel have also shown that protection against future infection is equivalent between vaccinated individuals and individuals who have acquired immunity naturally. Dr. Martin Kuldorff has written on this as well. However, universities have stated that immunity, demonstrated by positive antibody responses, do not count towards the vaccine mandate. If immunity doesn’t matter, what is the point of the vaccine mandate?
Mandates are unethical
The ethicality of vaccine mandates has been examined elsewhere in articles by a faculty person in philosophy and humanities, discussing the importance of not violating one’s conscience, and my previous article with an interview with Dr. Alvin Moss, the Director of the West Virginia University Center (WVU) for Health Ethics and Law.
In short, because these mandates threaten an individual’s education and/or career stability, they are coercive and impose an undue influence. Both of these factors violate informed consent, a keystone of medicine. My interview with Dr. Moss also tore apart other arguments in favor of mandates, such as “community ethics” and the idea that “public health ethics supersedes all other ethics.” This argument falls apart because the vaccine is not effective, as described above.
Another issue is that forced vaccines violate sincerely held religious beliefs. The Christian perspective on this is described nicely by the Warrenton Declaration, written by a group of pastors.
Last is the issue of risk. While public health professionals, academics, and health care professionals disagree about the degree of risk associated with these vaccines, the fact is that the risk is non-zero. Dr. Paul Alexander’s substack provides a succinct list illustrating these risks. One recent article suggested that the FDA glossed over important severe adverse effects associated with the vaccine.
Even the peer-reviewed scientific literature describes the severe reactions due to the vaccine. A systematic review of the literature summarized adverse reactions to the vaccine, including thrombocytopenia, thrombosis, anaphylaxis, and even death. While in many instances causality could not be proven, it could not be excluded either.
The authors stated that although these severe adverse events are rare, when a global population is exposed to this vaccine, the numbers could still be significant. Another mini-review adds pericarditis, myocarditis, and Guillain-Barré syndrome to this list of adverse reactions.
Most recently, a large national study in France, published in Nature Communications, found that vaccination with both these mRNA vaccines was associated with an increased risk of myocarditis and pericarditis within the first week after vaccination, and that this was most pronounced in younger individuals.
Further, these authors discussed that there is likely a causal link between the vaccine and these events. A recent article in the Brownstone Institute by Dr. Martin Kuldorff also closely examined the adverse effects associated with the vaccine. In summary, severe adverse reactions do occur, and might be more likely in younger (college-aged) individuals. When there is a risk of severe outcome in a population group where the COVID-19 infection fatality rate is low, vaccine mandates are unethical.
Mandates don’t even work
While there are likely many examples of the failure of vaccine mandates on college/university campuses, two are noteworthy. First, a tweet by Dr. Andrew Noymer, faculty at UC Irvine, presented that university’s COVID-19 dashboard, noting that in order to work at or attend UC Irvine, one had to be fully vaccinated and boosted with very rare exceptions.
Dr. Noymer’s tweet goes on to state that he in fact was both vaccinated and boosted, but also noting “It’s a big deal to fire someone. Doing so for such a leaky vaccine is not without its issues.”
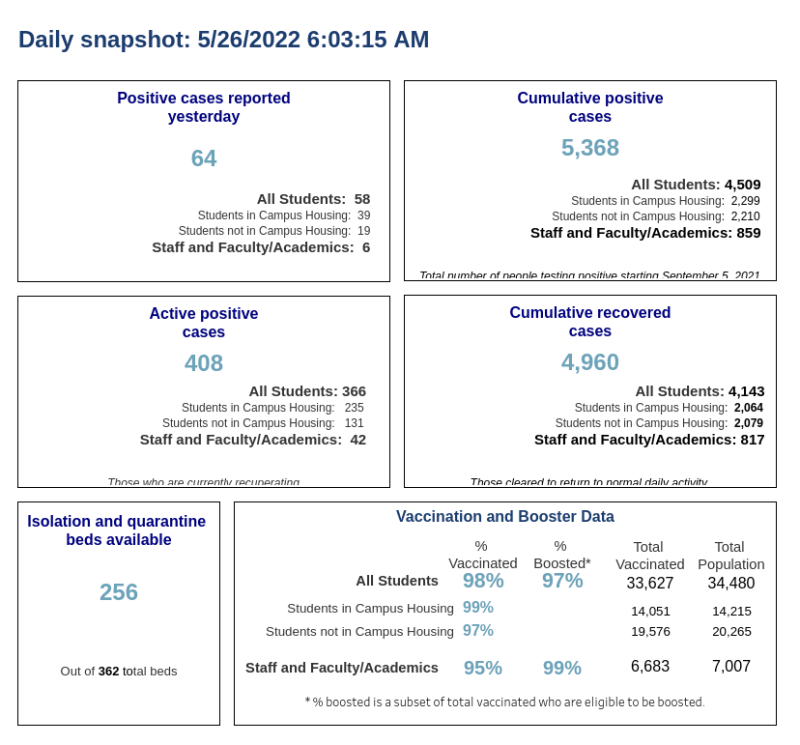
In another example, back in the fall semester, a twitter thread by Dr. Aaron Kheriaty put a spotlight on Cornell University, which shut down its campus due to high COVID-19 case counts . Dr. Kheriaty’s tweet stated that Cornell had a vaccine mandate, “purging” all unvaccinated students. The 3% positivity rate was called “significant” by the university’s president, but none of the cases were severe, and virtually every case occurred in fully vaccinated individuals.
These situations are similar to outbreaks reported on cruise ships. Cruise ships have extremely strict vaccine mandates, requiring all passengers to be fully vaccinated. And yet, a Carnival Cruise Ship that left Miami on April 17 was investigated for an “outbreak” because 0.3% of the people on the ship tested positive for COVID-19. Additional instances like this have been reported in the media. In sum, strict vaccine mandates do not result in zero transmission.
Conclusion
One of the most nonsensical aspects of continuing COVID-19 vaccine mandates is that individuals who survived the mandates last year – that is, were fortunate enough to be granted religious and/or medical exemptions – have to reapply this year.
Did these religious reasons suddenly change without the person complying with the mandate initially? Did these medical reasons that were severe enough to compel a physician to write an exemption suddenly go away?
Maybe either possibility did happen in some cases. But more likely, this is an exercise in obedience, or perhaps to wear down the morale of the individual. Both possibilities are not conducive to a healthy learning or working environment.
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.