
Can a single study provide insight — unintentionally — into all of the following aspects of the pandemic?
- Misclassification of non-Covid deaths as Covid deaths
- The “healthy vaccinee” bias
- Biases in vaccine effectiveness studies
- Short-term vaccine fatalities
- The death toll of Covid vis-à-vis the death toll of fear-mongering and “mitigation”
None of these topics is mentioned in a study from Israel, presented by researchers from Israel’s Ministry of Health. Yet all of them can be learned from their data.
In the imaginary world of Haklai et al. nothing ever goes wrong, as far as Covid is concerned. There is no misclassification of deaths, there are no biases that distorts estimates of vaccine effectiveness, and there are no deaths due to the disruption of normal life. Too bad their data provide evidence to the contrary.
The two components of the study are well-described by the authors:
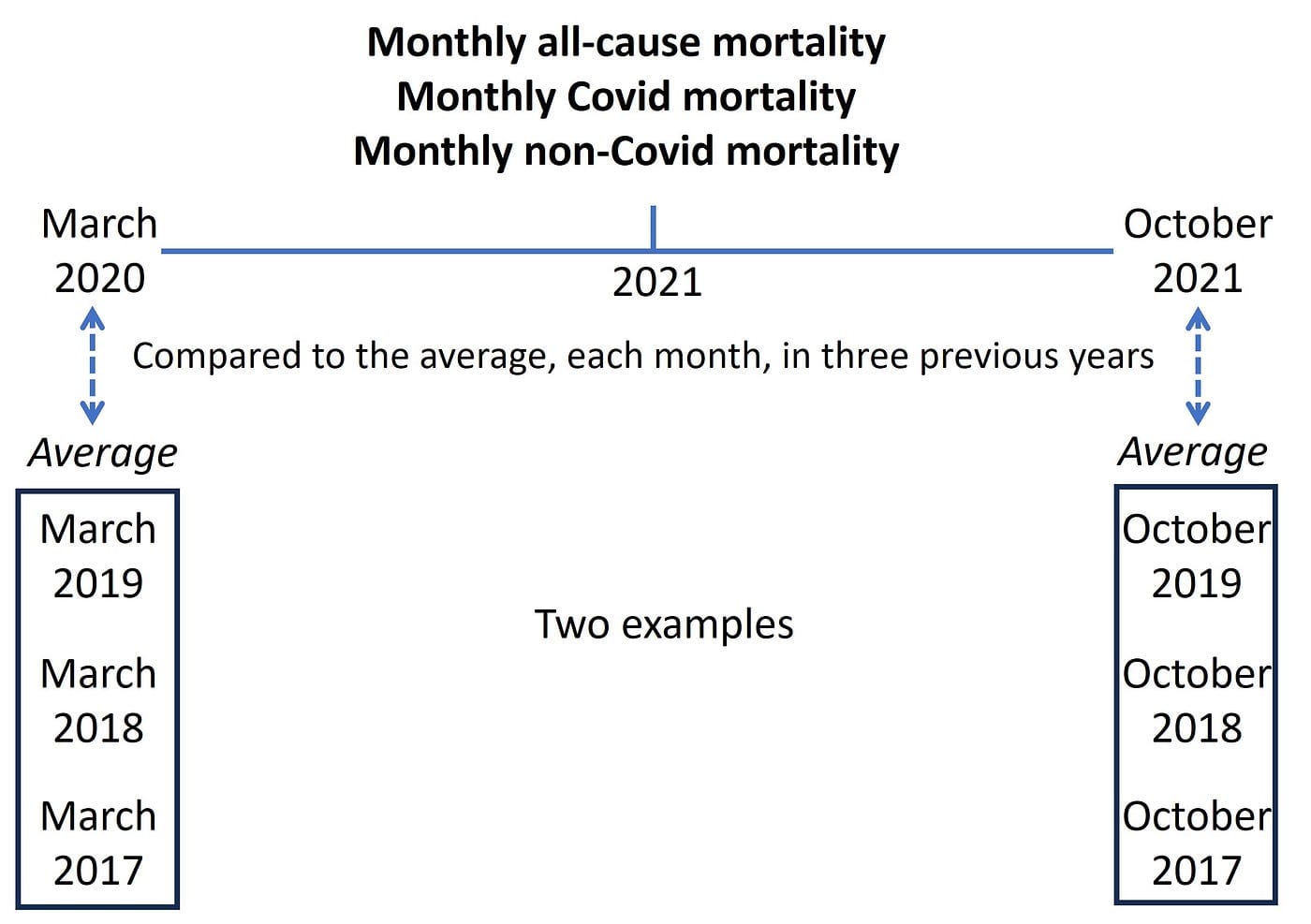
First, “We followed the total mortality rates and non-COVID-19 mortality rates in Israel between March 2020 and October 2021 compared to the average rates in 2017–2019, to assess trends in excess mortality, and COVID-19 and non-COVID-19 mortality by month…” [my italics]
My illustration:
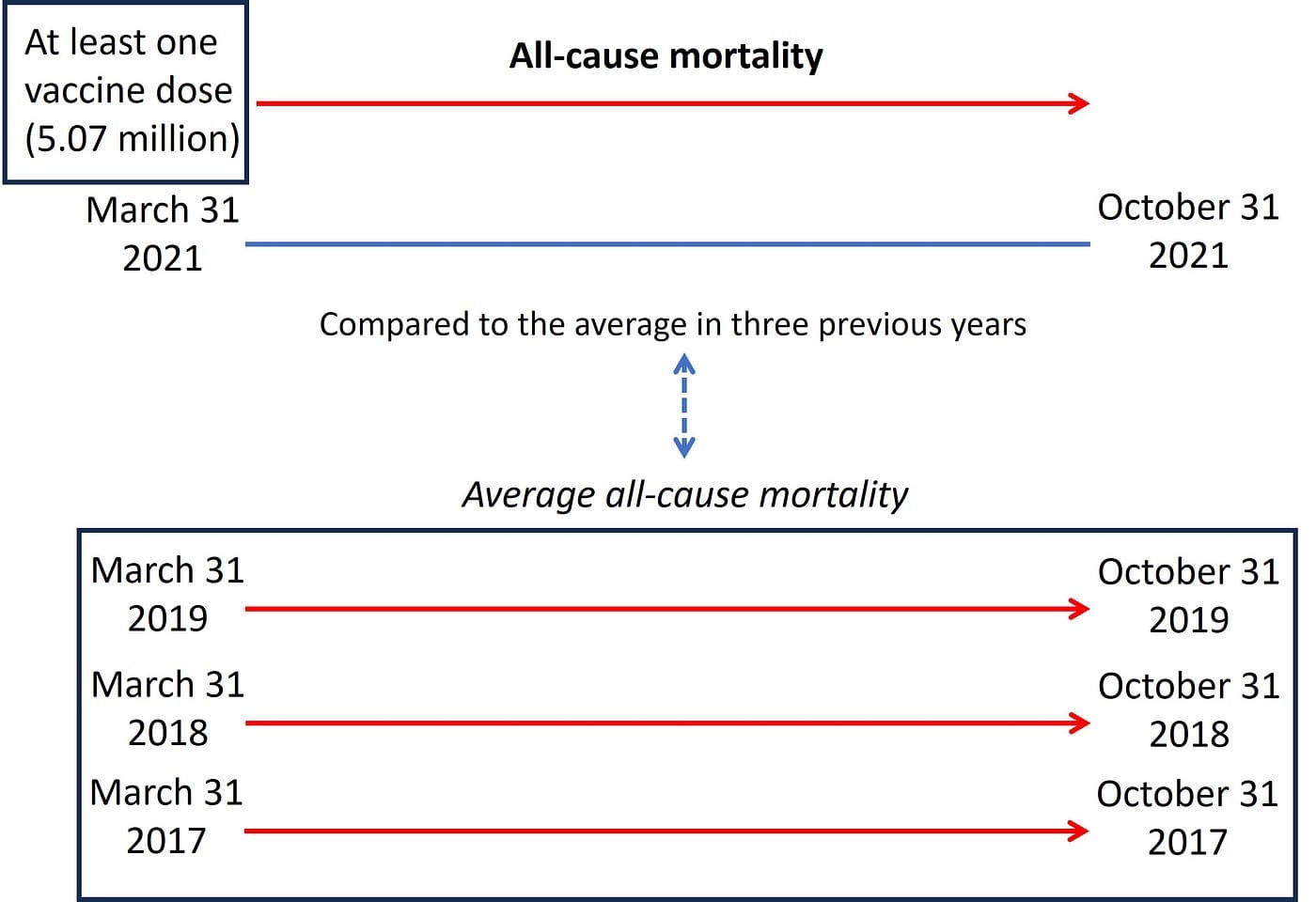
Second, “A cohort vaccinated at least once by 31 March 2021 was followed up for mortality in the following seven months compared to the corresponding months in 2017–2019.“
My illustration:
- Misclassification of deaths
The authors write: “….between November 2020 and March 2021, they [non-COVID-19 mortality rates] were significantly lower [than the average in 2017–2019]…”
Look at the height of the yellow bars during the Covid wave in that winter (rectangle added.) These bars reflect non-Covid deaths which were lower than expected (red line). Why would non-Covid deaths decline during a Covid wave? An epidemic or not, those who should die “normally” from various causes are not spared.
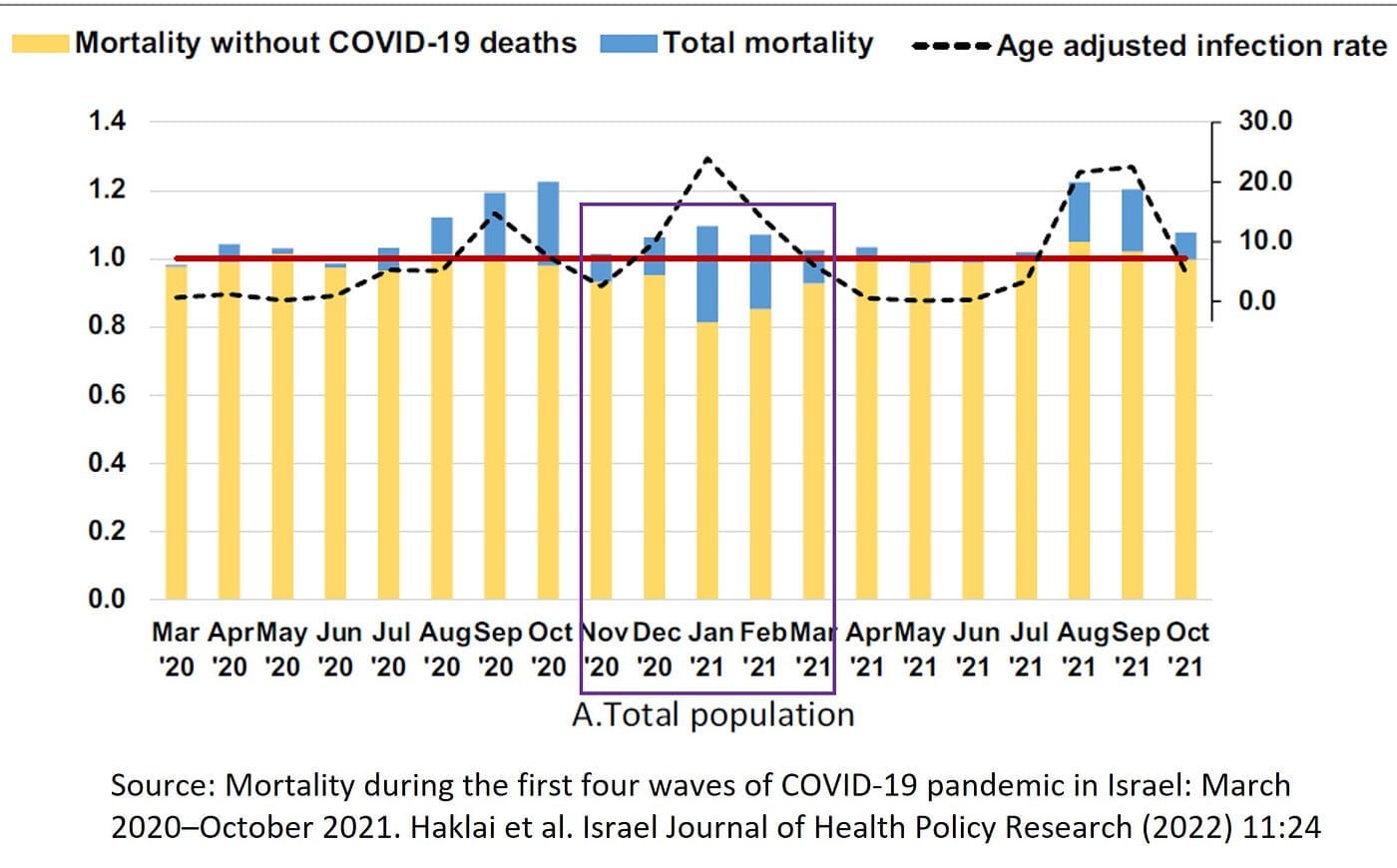
The answer is simple, much simpler than “mortality displacement” which the authors proposed. Deaths from non-Covid causes were misattributed to Covid. Deaths “with” Covid were counted as deaths from Covid (blue bars). That’s why the authors detect a “deficit” of non-Covid deaths (yellow bars not reaching the red line).
How severe was misclassification in that winter?
The bar graph indicates that it was severe, and a quantitative answer was provided by Israel’s Ministry of Health on its website.
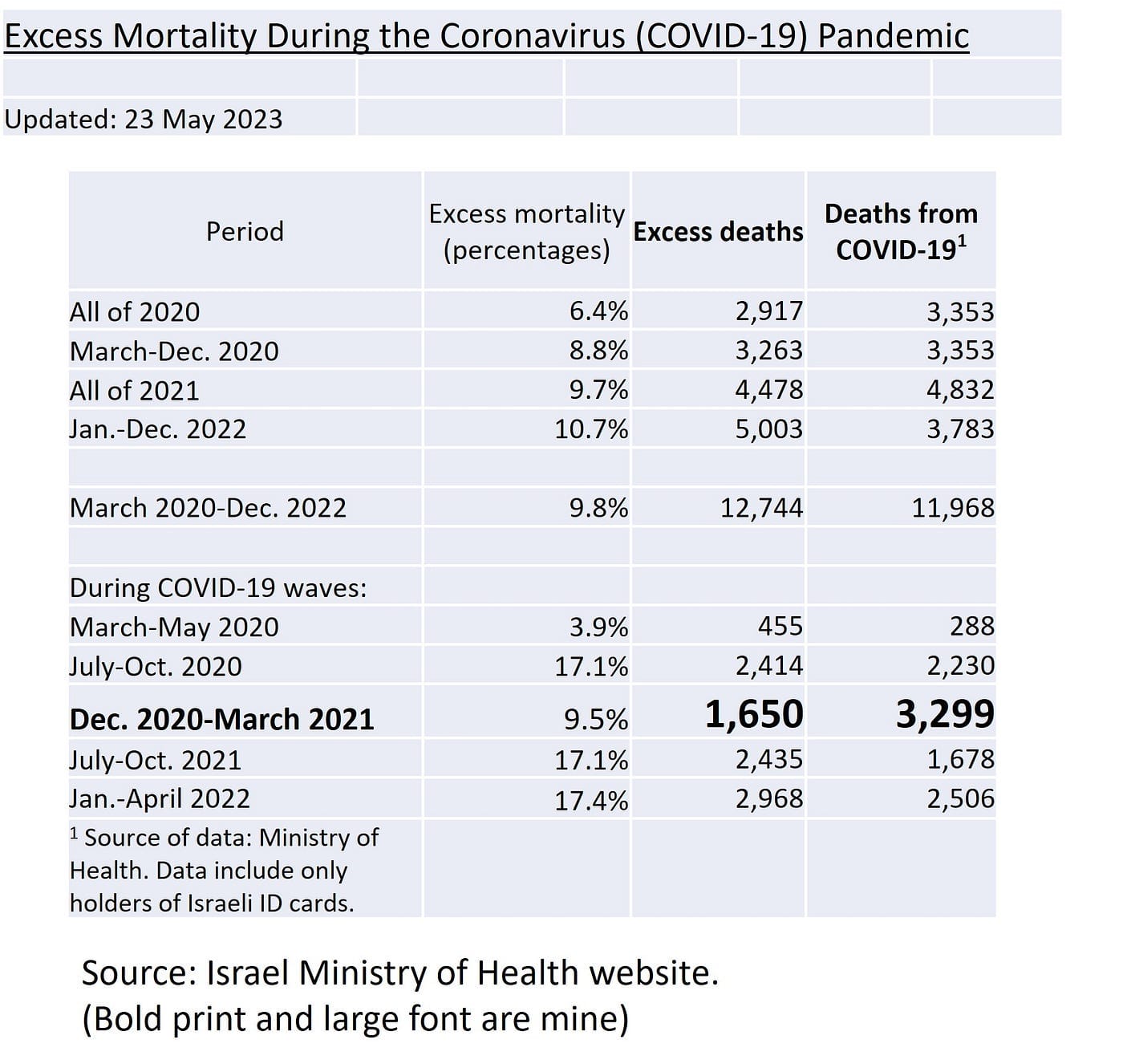
Between December 2020 and March 2021, there were 3,299 reported COVID deaths in Israel but the Central Bureau of Statistics (CBS) estimated only 1,650 excess deaths — half as many. For every true Covid death in Israel there was another so-called “Covid death” that did not account for excess mortality, which means that the person would have died, regardless of their positive PCR test. All those deaths should have been counted as non-Covid, shifted from the blue bars to the yellow bars.
Interestingly, that was also the level of misclassification in Sweden during the winter wave of 2020–21: nearly 7,600 reported Covid deaths, as compared with about 3,600 excess deaths.
What are the implications of such levels of misclassification?
First, during the winter of 2020–21 Israel served as the Pfizer laboratory for observational studies of vaccine effectiveness, which relied on reported Covid cases, hospitalizations, and deaths. Influential studies — on the basis of which billions have been vaccinated — should be retracted. No serious peer-reviewer would have allowed the publication of a study with 50 percent misclassification of the mortality endpoint. The results cannot be trusted.
Second, Covid mortality was overestimated.
Third, the split of excess deaths between Covid and the consequences of futile mitigation efforts is miscalculated. We’ll return to this point at the end.
2. Healthy vaccinee bias
The authors write:
“We saw no evidence of a deleterious effect of the vaccine as shown by mortality in the cohort of persons vaccinated at least once, over a seven-month period. On the contrary, we found lower mortality rates [as compared with 2017–2019].”
The rate ratios below compare all-cause mortality in the vaccinated cohort with mortality in previous years. Even if the Pfizer vaccine prevented all Covid deaths, we expect to observe rate ratios of 1, reverting the cohort mortality to the baseline rate of 2017–2019. Covid vaccines are not expected to reduce mortality from non-Covid causes.
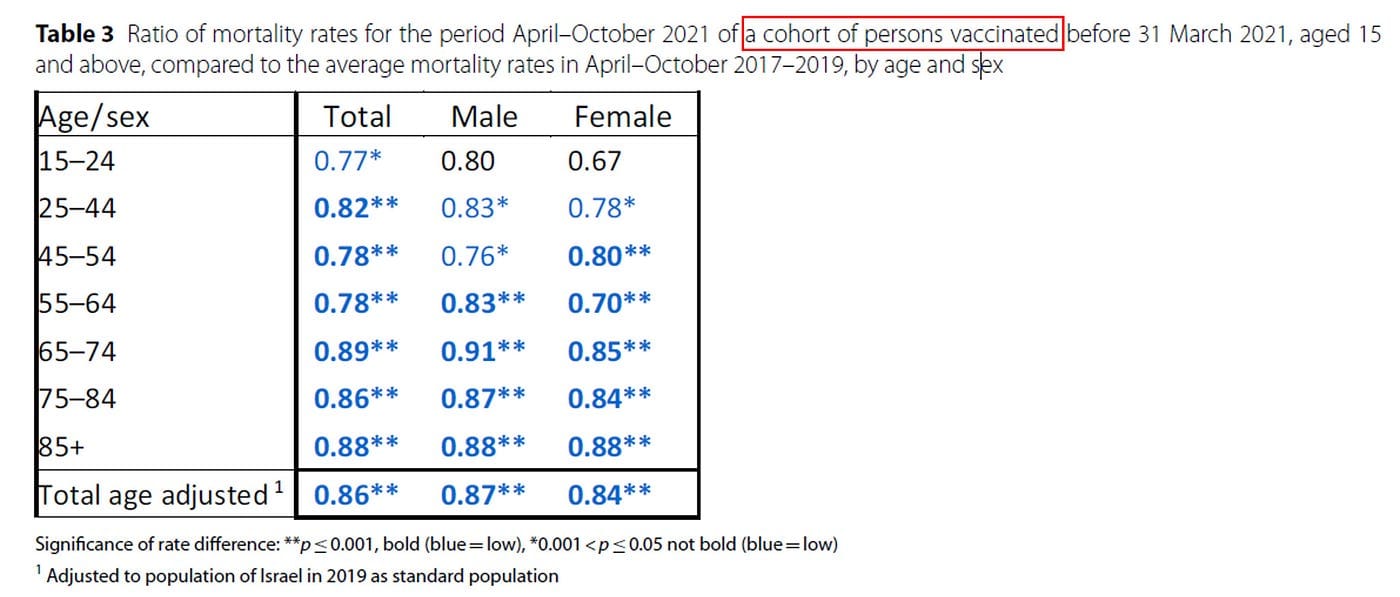
The authors write that “The lower rates may be due to the vaccinated cohort being a healthier population…” and they struggle with creative explanations.
The truth is simple. We are observing “the healthy vaccinee bias,” about which you can read elsewhere. Removal of the bias can change estimates of vaccine effectiveness from 85–95 percent to null or worse.
An interim summary:
Vaccine effectiveness studies from Israel embed at least two major biases: severe misclassification of the mortality endpoint and the healthy vaccinee bias. Neither is mentioned in the paper. And two other biases might have operated.
3. Booster fatalities
The booster campaign in Israel began at the end of July 2021, concurrent to a rising Covid wave (Delta).
The authors write: “…a first booster shot was administered to the public starting at the end of July 2021, which helped to bring this wave under control by November 2021.”
That’s an interesting inference. Do they assume that Covid waves never end naturally?
Whether the booster had any significant effect on Covid death is debatable. On the other hand, there is evidence of short-term fatality, as explained next.
The authors note one exceptional observation, which I highlighted in the figure below (arrow):
“Only in August 2021 was the rate of non-COVID-19 mortality significantly higher than 2017– 2019, 5% (95% CI 1–9%) higher for the total population.”
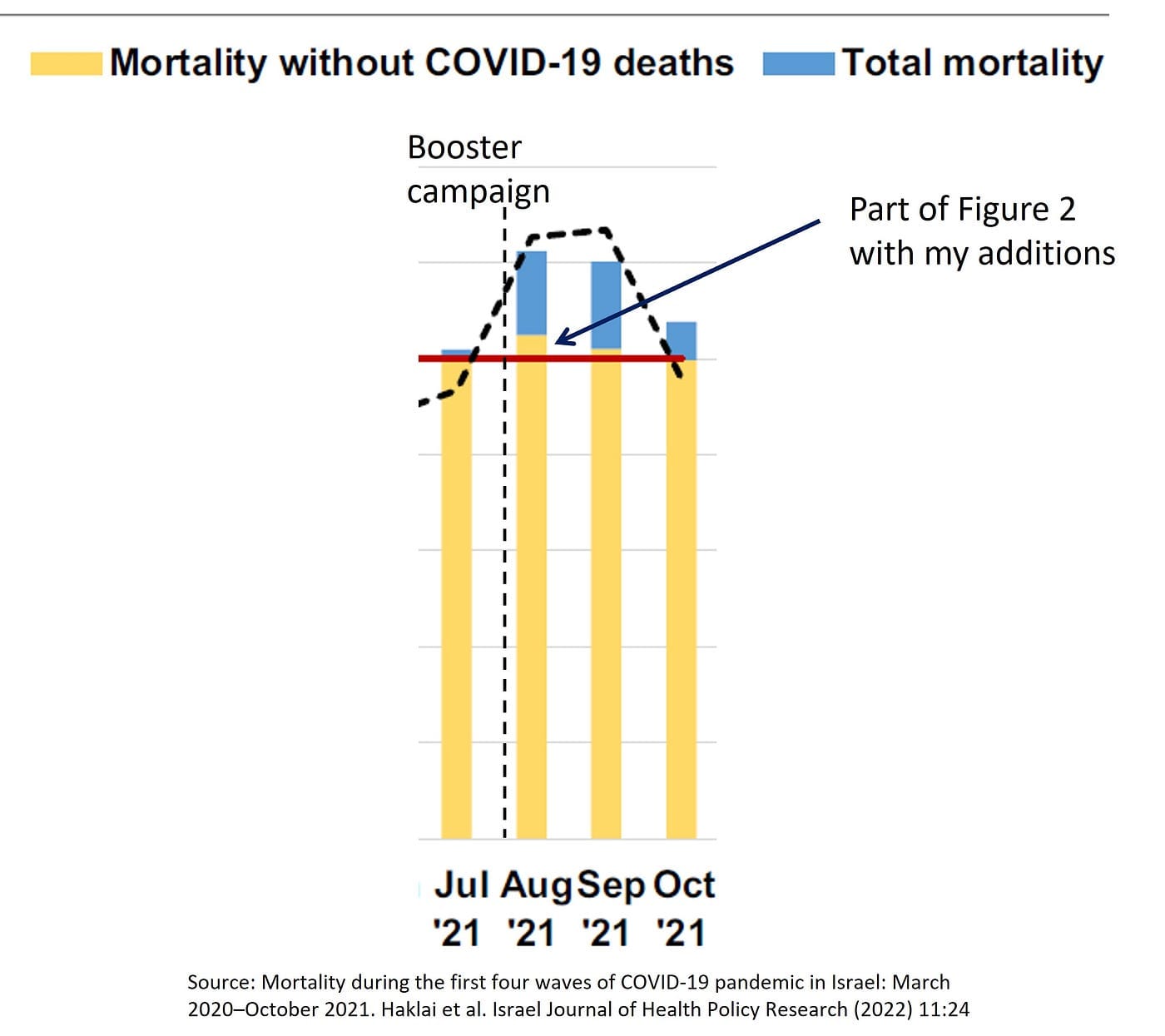
This anomalous excess is compatible with vaccine fatalities in the most vulnerable population, which was vaccinated first.
How many deaths make up 5 percent excess non-Covid mortality cannot be computed from their monthly data, but it is probably close to 200. If misclassification of non-Covid deaths as Covid deaths persisted in August 2021, excess non-Covid deaths should have been higher.
Elsewhere, I discussed uncertainties and concluded that the number of booster fatalities in August 2021 might have been 200 to 400, which is a conservative range.
4. The death toll of fear-mongering and “mitigation”
The authors write:
“Between March 2020 and October 2021 there were 84,124 deaths in Israel giving an excess of 8953 deaths compared to the average of 2017–2019, slightly higher than the number of deaths attributed to COVID-19 in this period, 8114.”
First, that’s 12 percent excess mortality over a 20-month period, worse than in lockdown-free Sweden.
Second, that “slightly higher” number of excess deaths than Covid deaths is 10 percent higher (839/8114). But as we now know, the number of true Covid deaths was substantially lower than 8,114 Covid-attributed deaths.
A little math:
Over the study period, non-Covid mortality was lower by about 3 percent than the average in 2017–2019 (Table 2 in the article.) That’s about 2,200 “missing” non-Covid deaths, or rather 2,200 deaths that have been misattributed to Covid. If we add 2,200 (misattributed) to 839 (the difference between excess deaths and reported Covid deaths), we get about 3,000 excess deaths that are not accounted for by Covid. That’s one-third of all excess deaths in Israel(3,000/8,953).
But let’s choose a conservative set of assumptions:
Only 1,650 deaths should be shifted from 8,114 reported Covid deaths to the non-Covid rubric. That’s the number of non-Covid deaths in the winter of 2020–21 that were mistakenly attributed to Covid, based on excess mortality (Section 1, above.)
Let’s add 150 Covid deaths that might have been missed during the minor, largely inconsequential first wave.
On these assumptions, 12 percent excess mortality in Israel (8,953 deaths) is split between 9 percent excess Covid mortality (6,614 deaths) and 3 percent excess non-Covid mortality (2,339 deaths). Non-Covid causes accounted for 26 percent of excess deaths.
In summary, between one-quarter and one-third of the excess mortality in Israel during the study period was not Covid.
What has caused it?
An American journalist once wrote that unaccounted excess deaths were related to “the circumstances of the pandemic.” These circumstances have been created by officials in Israel and elsewhere: panic, fear-mongering, lockdowns, disruption of normal life, coerced vaccination — with all of their consequences, including death. None of that happened in a previous pandemic. Chances are that destructive interventions will be implemented again in a future pandemic, in the name of public health.
In a section titled “Health policy implications” the authors write:
“We found that in Israel the excess mortality was similar to the deaths attributed to COVID-19 mortality, unlike in many other countries.”
That sentence should be revised, replacing “attributed” with “attributed and misattributed.” As for similarity, check what true similarity looks like (scroll to the last table, rightmost column.)
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








