
It’s starting to look like New Zealand’s Ministry of Health makes a habit of undermining democratic process in order to skirt around inconvenient truths. The New Zealand Bill of Rights Act 1990 (BORA) could be collateral in the game that is being played. But it’s bigger than that.
Members of Parliament, officials at the Ministry, and affiliated agencies are prepared to write out public concerns about health risk from forced medicalisation in public consultation processes. The Ministry is aware that public trust is declining, because they’re constructing coercive frameworks to ensure that affected actors comply. No matter the evidence as to safety.
Mandating a medicine should require a higher bar because it impacts upon human rights. But the undermining of democratic process is greater than that. New Zealanders can observe poor process in laws passed requiring the fluoridation of drinking water as well as in the locking in of Covid-19 mandates in New Zealand.
In parallel we observed the weaponisation of selective science and exclusion of peer-reviewed science; a gaming of public submission processes; and the deployment of punishing consequences for those who do not acquiesce.
A November New Zealand High Court judgment concerned a decision to fluoridate drinking water. The then Director General of Health, Ashley Bloomfield, was found to have failed to take into account the New Zealand Bill of Rights Act 1990 (the Bill of Rights Act) which ensures the right to refuse medical treatment.
When a decision has the potential to restrict a fundamental right in BORA, officials must thoroughly consider that restriction and consider whether it is demonstrably justified in a free and democratic society.
The judge found that enforced fluoridation was a reasonable limit on rights; therefore the Director General made an error of law in failing to take into account and give due weight to BORA.
We might presume fluoridation of drinking water is, as Bloomfield maintained, safe and effective. Yet in order to arrive at this presumption, the Ministry of Health – and Parliamentary – processes and practices inevitably write out inconvenient considerations. By excluding important issues, or relevant considerations, risk of harm might be minimised. However, this occurred throughout Covid-19 as mandates rained down on healthy people.
Perhaps compulsory or mandated medicine is better described as command medicine.
Coercion is at the forefront. In the case of fluoridation, local councils that do not comply within the specified timeframe are faced with a fine of NZD200,000 and then NZD10,000 for each day the fluoridation equipment is not operative.
New Zealanders who resisted the BNT162b2 vaccine lost their jobs and their access to public places.
In the case of fluoride, the Crown was concerned with an ‘overburdening of the administrative decision-making process.’ But of course, process shapes outcomes. What we consider or don’t, what is relevant, is material to an outcome.
Flouride
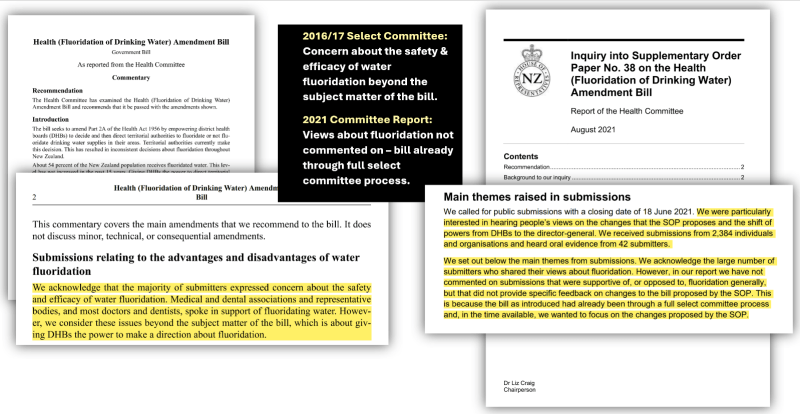
As a background to the November High Court judgment, in 2016 the Ministry of Health decided to shift the power to District Health Boards to decide whether to fluoridate local drinking water. That Amendment Bill stalled after the Select Committee process in 2017. Then in 2021 it was picked up again as Supplementary Order Paper No.38, this time transferring power to the central government. Now, the Direct General could direct local suppliers to fluoridate drinking water.
In both the 2016 Select Committee process, and the later 2021 Inquiry process the public was invited to comment. No risk assessment was undertaken by the New Zealand Environmental Protection Authority, nor any other New Zealand regulator. Yet all public comments concerning the safety of fluoridation were dismissed by these committees unless they directly addressed the legislation text.
I’m a trustee of Physicians and Scientists for Global Responsibility (PSGR), and our 2021 submission emphasised that the
potential for dental caries to be alleviated by fluoride in some groups, appears outweighed by the uncertainty concerning life-long health risks to both unborn babies through to 6-year-olds.
PSGR emphasised that there are particular windows of vulnerability at this young age that must be considered. Five-year-olds in New Zealand have higher levels of fluoride in their bodies than adults. PSGR’s submission also drew attention to the accumulated risk from fluoridation to thyroid health, risk for arthritis, and ADHD.
We were soundly ignored. The bill had been through the full select committee process. Chair Liz Craig and colleagues omitted to mention that the public was soundly ignored in 2017 as well.
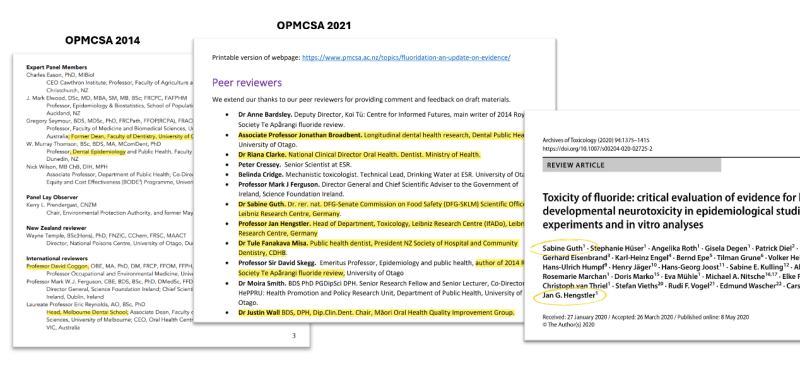
In the letters directing local councils to fluoridate, the Director General cited three documents as sufficient scientific evidence for fluoridation. A 2014 and 2021 Update by the Office of Prime Minister and Cabinet’s Chief Science Advisor (OPMCSA); and a 2015 Cochrane Review (where the only risk considered was of dental fluorosis).
The 2021 OPMCSA Update suggests a predetermined position. As I have discussed, peer-reviewers included authors widely cited in that same 2021 Update.
There was no methodological review of the literature to ensure that any assessment was impartial, and the OPMCSA did not assess the lowest level of safe exposure. In fact, to date, because fluoride hasn’t undergone risk assessment, there is no known safe level of exposure. Keep in mind that the 1.5 mgL guideline level was established in 1984, the ‘optimum level’ in 1957, and that Europe’s acceptable intake levels are based on epidemiological studies from the 1970s.
The OPMCSA concluded ‘that there was no convincing evidence of neurological risks.’ Their claim has been contradicted by US National Toxicology Program (NTP) scientists who refused to rule risk at claimed safe levels of exposure because the evidence is uncertain at these levels, and therefore harm could occur.
Any risk-benefit claim stood on shaky ground. Neither the Ministry of Health, nor the OPMCSA conducted an analysis to balance risk by age and health status, particularly the economic and social consequences of long-term loss of IQ following exposures in early childhood.
Covid-19
As process informs outcome, what happened as mandates were rolled out for Covid-19? Vaccination-for-all policy had been established in March and April of 2021. As was done with fluoride, officials wrote public concerns out of the Select Committee process.
By April 2021 New Zealand authorities would have been informed that Pfizer’s BNT162b2 vaccine was found to cause an extraordinary range of adverse events. We now know that the CDC in April 2021 was receiving accounts of breakthrough infections in the very population that should have been most protected, nursing home residents.
But this critical information was never communicated by New Zealand legacy media. Despite New Zealand claiming to be informed by other regulators, it seems that bad news of a medical intervention that was not as good as it was stacked up to be was harder to filter out.
Of course, a year earlier, in April 2020 it was known that SARS-CoV-2 did not pose a risk of hospitalisation and death for the majority of the population, and indeed, generally older populations were not at the severe risk talked up by governments. Those at extreme risk were nursing home residents and people with chronic complex metabolic conditions.
I’ve spent some time understanding the gap where the government should have reviewed the published literature to triangulate corporate claims that Pfizer’s BNT162b2 vaccine was safe and effective. In the information void, the TAGs, the Technical Advisory Groups, and the Department of Prime Ministers’ modelling groups produced information that ushered in vaccines-for-all and failed to consider risk by age and health status. Information that contradicted this was strangely written out.
The October Protection Framework may have been only poorly supported in law. When Covid-19 Minister Chris Hipkins released the COVID-19 Amendment Bill (No.2), Attorney-General David Parker was required to consider the New Zealand Bill of Rights Act 1990 (BORA). In September 2021 he declared that changes to Hipkins’ Amendment Bill (No.2) would not impact human rights. But there was no specific analysis of whether mandatory vaccination would constitute an infringement. Parker avoided discussing mandatory vaccination specifically as a human right infringement.
Parker was not an impartial actor. He introduced and oversaw the Secondary Legislation Act (which smoothed the Orders process) and oversaw and introduced the overnight COVID-19 Public Health Response Act 2020. This was the principal Act that was being altered by the Amendment Bill (No.2). Parker was a member of Cabinet. Cabinet collectively initiated legislation and approved secondary legislation. Parker was closely involved in Covid-relevant legislation.
I speculate Parker knew precisely when the April 2021 rollout frames were scheduled. He arguably lacked the independence necessary for making human rights-related decisions on behalf of people and their Parliament.
Surprisingly, Hipkins’ Amendment Bill (No.2) barely mentioned vaccines. Instead, it created the framework that enabled a further Act and then a raft of unfettered secondary legislation to be produced secretly through Cabinet, as Orders in Council. In a short space of time, this secondary legislation would demand that New Zealanders succumb to vaccination to retain their employment, access to public utilities, and their social life.
Amendment Bill No.2 contained only a single reference to vaccines. Yet in the short consultation period, only ten days, 14,626 people submitted to the COVID-19 Amendment Bill (No.2), most protesting further stringent measures, including vaccine mandates.
When public submissions closed, the Ministry of Business, Innovation and Employment strangely and swiftly stepped in to produce an October 2021 Departmental Report. This report acknowledged that
Many submitters expressed concerns that Government would have an unfettered ability to require mandatory vaccination, detain the unvaccinated, subject people to compulsory medical testing, examination or experimentation, or otherwise infringe their human rights without justification.
The following Health Committee report did not discuss public concerns about the safety and efficacy of the vaccine and the moral and ethical issue of mandates.
Hipkins’ COVID-19 Public Health Amendment Act (No 2) came into force on the 19th of November.

The public could not know that Hipkins and the Crown Law Office were, in parallel, beavering on COVID-19 Response (Vaccinations) Legislation Bill, even as Amendment Bill (No.2) was being consulted on.
The Amendment Bill (No.2) became law on November 19. One working day later, Hipkins quietly introduced another amendment bill, the COVID-19 Response (Vaccinations) Legislation Bill. Hipkins’ 5,500-word bill was passed in one day, becoming law on November 25. We presume that this Bill was being drafted in October or before. This time, vaccine/vaccination was mentioned over a hundred times.
One day later, November 26th, the first COVID-19 Public Health Response (Vaccinations) Order 2021 became law, a 12,000-word tome. I’ve asked for the date the Crown Law Office commenced drafting the vaccinations legislation, but they won’t divulge it. Vaccine mandates surged out, lobbed like hand grenades into the lives of generally healthy people, because, by December 3 all who wanted to enter a place or receive service were legally required to show their Covid-19 vaccination certificate (CVC).
The public suspected that mandates would be formalised via Hipkins’ legislation. They were correct. At this point in time, there were myriad published reports of vaccine breakthrough and extensive reports of harm caused by the vaccine. The Alert system had ended, replaced December 3 by the COVID-19 Protection Framework.
Patterns Repeat – What About the Global Pandemic Treaty?
Perhaps compulsory or mandated medicine is better described as command medicine.
In last weeks’ fluoridation decision, the judges concern was whether BORA was taken into account for mandated medicine in drinking water. In 2021, the Attorney-General failed to consider mandated medicine (vaccines) in his BORA assessment. We may be looking at experts with a predetermined view. Why didn’t the peer review process for the OPMCSA’s 2021 Update include experts in neurotoxicity? During Covid-19 the TAGs produced science to support vaccination, while dissenting epidemiologists were silenced and ignored.
Select Committee processes have persistently failed to address public concerns about risk from fluoridation and the BNT162b2 gene therapy. New Zealand officials have not taken steps to impartially review the scientific literature. The public, stepping in to shed light on the gaps, has been ignored and dismissed.
These patterns suggest we step away from the World Health Organization (WHO) amendment and Pandemic Treaty process. Why? We’ve observed how swiftly the Ministry of Health accelerated compulsory vaccination through the secret secondary legislation process, while developing onerous fines if councils hesitate to fluoridate.
An extraordinary compendium of papers will bind us to WHO decisions and create pathways to legitimise more compulsory surveillance and compulsory medicine, and the digital infrastructure that will weaponise UN-based global responses. The devil is in the detail. They contain ample space for problematic and largely unforeseen risks and challenges that might apply to New Zealand. From the WHO CA+, the “Proposal for negotiating text of the WHO Pandemic Agreement,’ to the Political Declaration on Pandemic Prevention, Preparedness and Response.
Equity (to the tune of $30 billion) is based on vaccines, diagnostics, and therapeutics. That’s why I have co-signed a letter asking that the Attorney-General and the Human Rights Commissioner take this seriously, because the Cabinet hasn’t.
Dauntingly, in front of us sit 307 Amendments to the 2005 International Health Regulations. Immediately and most urgently are Article 59 IHRAs which shorten timelines for rejection or implementation of those future IHRAs… more than 307 of them. But of course, the Cabinet is uninterested – even when the number and scope are mind-boggling.
Equity sounds moral and ethical. But it’s medical greenwashing when everyone is mandated. Because not everyone is at risk of that outcome, and every human body will differently cope with a synthesised, chemical or biologic compound.
Public health is in a state of crisis, and in this crisis, the WHO is prioritising rare pandemics, and failing to address more urgent demands. Their obsession around surveillance, medication, and digital infrastructure reflects the priorities of their corporate funders. It arises from pervasive and entrenched conflicts of interest.
There’s no intention nor resourcing in these WHO documents to take measures to reduce the preventable chronic disease burden that vastly increases risk in an infectious disease epidemic.
The WHO, mind you, is still able to declare a pandemic based on the infectiousness of a viral agent, rather than its capacity to hospitalise or kill people. This attitude gave governments the rationale to demand that healthy families and teenagers be injected with an experimental cellular gene therapy, that had never undertaken toxicity testing for genotoxicity or carcinogenicity; or even, troublingly for a biologic drug prone to contamination, testing by batch before release of RNA or DNA contamination.
Mandated or command medicine policies are authoritarian. They are totalitarian because in deploying the related technology, digital or medical, they cooperate with a massive array of commercial providers, with most arrangements undertaken in secret.
They fail to require equal consideration for less risky interventions at every age and health status. They dismiss and ignore public appeals to consider the published scientific literature. The absence of broader consideration sets the stage for overreach and abuse of power at scale and pace.
What we see in command medication and digital is a general failure to require and include in these policies a place for the production of scientific information that might challenge or contradict claims of safety. The feedback loops are simply not there, they’re not sophisticated enough, nor open and transparent enough. They never will be. The distance between Geneva and Otago is far too vast.
We can envisage human rights as collateral at scale and pace, should the WHO and UN agencies gain such powers.
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








