You are an otherwise healthy person, and you want to keep it that way.
However, wherever you turn you are being told that your current state of ‘health’ is tentative; You could be sick and not know it. Maybe you have something lurking inside — possibly an early sign of cancer — so shouldn’t you do something? After all, better safe than sorry, right?
Consider this statement from Dr. David Sackett in The Arrogance of Preventive Medicine, CMAJ Aug 20, 2002:
Preventive medicine displays all 3 elements of arrogance. First, it is aggressively assertive, pursuing symptomless individuals and telling them what they must do to remain healthy.
Second, preventive medicine is presumptuous, confident that the interventions it espouses will, on average, do more good than harm to those who accept and adhere to them.
Finally, preventive medicine is overbearing, attacking those who question the value of its recommendations.
We have whole industries set up to discover potentially deadly cancers inside our breasts, prostates, lungs, cervixes or colons and your doctor, ever helpful and concerned about your future, suggests that you submit to screening. Guidelines recommend it, influencers push it and “survivors” preach of the benefits of screening.
“Better Safe than Sorry” is not just an axiom that rules our lives, it is frequently unchallengeable. After all, only an idiot would avoid early cancer screening, especially if such screening could save their lives, right?
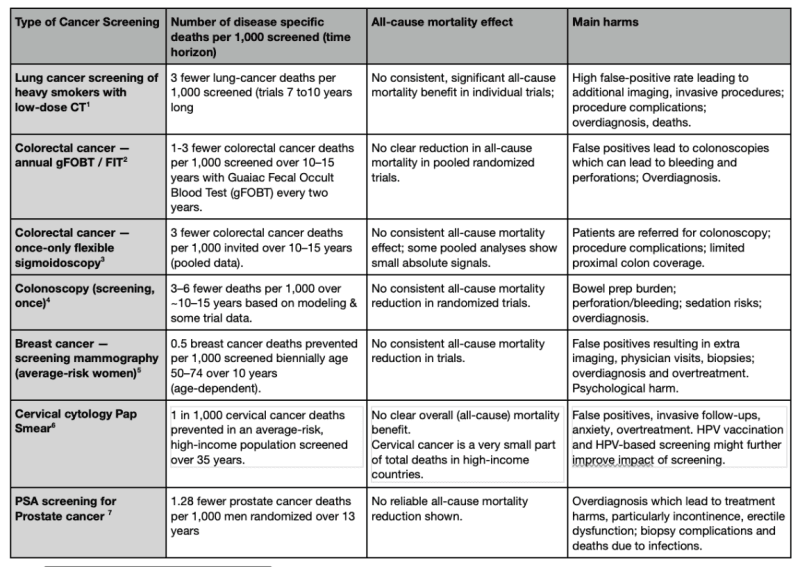
Let me be the bearer of blunt news: Cancer screening in otherwise healthy people doesn’t save lives. We’ve been sold a bill of goods by screening industries consistently overselling the benefits and underselling the harms. Those promoting screening boldly declare that the war on a specific cancer is being won, even though the data doesn’t show that screened patients live any longer than unscreened. Looking closely at the evidence of established screening programs drawn from randomized trials and meta-analyses of thousands of healthy people, you find that screening breasts, lungs, colons, cervixes, or prostates are good at finding early signs of cancer, but that detection doesn’t lead to lower overall death rates. (see table below)
Let me be clear to whom I’m speaking: healthy people. If you are a person with any symptoms, or perhaps even a family history that might suggest you would be at higher risk of certain types of illness, asking for screening might make sense. But I am talking about otherwise healthy people who are living their lives perfectly well, but told that by submitting to a screening test (of whatever organ) they are going to live longer.
Mammography is proven to save lives, right?
Let’s take the one cancer screening program that has the best, and most robust evidence from dozens of high-quality randomized trials: mammography. The most basic assumption with mammography is that it will find small, treatable cancers in the breasts of otherwise healthy, symptom-free women, and save their lives by stopping those tumors from growing into larger malignant cancers that could kill them. This is a very appealing assumption that drives the whole machinery of mammography.
However, the largest screening trials repeatedly show that any reductions in breast cancer deaths are not matched by fewer deaths overall.
One large trial analysis showed that the cumulative risk of breast cancer death to age 60 was 0.53% with mammography vs 0.48% without, an absolute difference of 0.05 percentage points. This means that for every 2,000 women invited for screening over 10 years, one will not die from breast cancer. There is however, no difference in death rates between screened groups and unscreened groups. Oh, and before we forget to mention, along the way, it also means that at least 10 healthy women out of those 2,000 will be treated unnecessarily.
What is going on? Commentators have suggested two possibilities: the trials were too small to detect an overall benefit. Or screening just shifts harms to other kinds of deaths, due to complications, other cancers or cardiac deaths.
I feel that if they can’t find an overall mortality benefit in studies involving tens of thousands of women in high quality randomized screening trials there probably isn’t one. The implications of this are shocking.
Screening finds early signs of disease but it also manufactures patients. False positives trigger cascades of medical busyness and interventions—trips to the doctor and clinics, repeat imaging, biopsies, invasive procedures, pathology reports, and the diagnosis of conditions that would have never gone on to hurt you. The impact on a person’s life can be catastrophic to say the least, and all the tests, clinic visits, chemotherapy, surgeries and drugs all come with a cost and harm to patients and to health systems.
Each step multiplies costs and complications. Many people endure months of insufferable anxiety after a scare, only to learn later they were healthy.
Yet the mammography screening programs push on, and a defensible conservative estimate is that the mammography-to-treatment cascade costs roughly $13 billion–$16 billion in the U.S. each year in direct health care spending. The biggest chunk of this is the screening services themselves, the downstream diagnostic workup (diagnostic mammograms, ultrasounds, biopsies), with the rest coming from the screening exams plus the treatments (surgery + radiation). Add into this all the drugs and surveillance imaging and we’re talking big money.
Then there is the belief, where every woman who has been through a lump-detected hell comes out the other side as a champion for screening everywhere. Even if she was just another victim of an imperfect cancer-detection enterprise.
And that’s just breast cancer.
When you crawl into the evidence of screening for prostate cancer, cervical cancer, colon cancer and lung cancer, does the story change?
Sadly it does not. Those forms of cancer screening, also sold as “better safe than sorry”, can find early signs of cancer. Some lives are ‘saved’ due to treating the cancer they were looking for, but on balance screened patients don’t live any longer than those not screened. And likely the quality of their lives has decreased.
The enormous sums to fund cancer screening industries do not float in a vacuum — they come from finite health budgets, clinician time, hospital capacity, and public trust. Every dollar sunk into routine surveillance of the “not-yet-sick” is a dollar not spent on people who are manifestly sick and whose outcomes would measurably improve with better access to diagnostics, treatments, palliative care, and social supports.
Dr. David Sackett, considered the father of modern evidence-based medicine, could have been talking about cancer screening when he railed against the arrogance, of “preventive medicine” being practiced today. The cultural messaging — pink ribbons, celebratory narratives of “finding it early” — and the assertiveness around taking complex, risky health engagements and framing them as civic duty. Many who undergo screening do so out of fear and obligation rather than informed consent. Most people will have heard the story that “a mammogram saved my sister’s life” without knowing that ten other sisters have had their lives turned upside down unnecessarily. When the evidence base is uncertain or negative for mortality benefit, continuing mass screening seems a strong ethical breach: it binds healthy people to medical surveillance that creates harm and dependence, without clear benefit.
What reforms would I suggest?
I would put the brakes on all routine population-wide cancer screening programs and move resources to places where they would make a difference. I’d start by putting some teeth into “shared decision-making” using reliable statistics that clearly lay out the likelihoods of benefit versus harm for all healthy people undergoing screening. Until screening shows net lives saved and net benefit to people — not just to certain death-certificate tallies — coercing people into getting screened should not be standard practice.
I’d make sure any savings are directed to timely diagnosis and treatments for symptomatic people, and improvements in the social determinants of health that we know are responsible for many avoidable and fatal diagnoses, including cancer.
I’d force health systems to fund independent, I’d force health systems to fund independent, impartial trials focused on what we suspect are real causes of cancer: food additives, chemicals, pharmaceuticals and electromagnetic radiation, for starters. I’d make sure that health systems everywhere were funding trials focused on all-cause outcomes, quantifying screening’s benefits and downstream harms including psychological distress, procedure complications, and economic cost.
Reform must come with two things: humility and sympathy. We need the humility to agree that any preventive treatment, while potentially beneficial, comes with harms.
We must agree that being assertive, presumptive and overbearing is no way to sell medical screening.
But also we must be sympathetic to those who were sold a bill of goods. People who believe that eternal medical vigilance equals virtue are not dumb, but they have been misled. And those who now live under the cloud of surveillance deserve compassion, not blame. We framed screening as prevention; instead, it has become a factory of medicalization, anxiety, and expense. If medicine’s moral compass is to be preserved, we must close the assembly line.
References
- NLST (Aberle et al., N Engl J Med 2011); NELSON (de Koning et al., N Engl J Med 2020)
- Multiple randomized FOBT trials; Cochrane/systematic reviews
- UKFSST, NORCCAP, SCORE, pooled RCTs
- NordICC randomized trial; modeling (MISCAN)
- Major RCTs, USPSTF/CISNET modeling
- Raffle, et al BMJ, 2003
- ERSPC (Schröder et al., Lancet 2014 update); PLCO
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








