
In a historically embarrassing decision, the FDA recently became the only international regulatory body to authorize the use of mRNA vaccines from Moderna and Pfizer for children aged six months to five years.
For the overwhelming majority of young children and toddlers, there is likely no justification or need for this concerning authorization.
They are at vanishingly small risk of serious complications from COVID, meaning that the risk-benefit calculation is precarious at best, and potentially negative at worst.
It’s also a testament to the disturbingly successful politicization of the US regulatory agencies that essentially no other internationally respected country anywhere on earth has made this bewildering decision.
Sweden, for example, has stopped the rollout of the Moderna vaccine for anyone under 30.
Not 18. Not 12. Not 5. 30.
The United States is now going to be vaccinating children as young as six months old with the same product that Sweden has banned for use in anyone under 30, citing side effects that tilt the risk-benefit numbers.
Despite this concerning difference of opinion, the White House Chief of Staff/Acting President Ronald Klain confusingly celebrated the announcement:
Interestingly, The New York Times link Klain tweeted brought up yet another concerning aspect of the authorization process, requiring an examination of the FDA’s documents and past statements.
The first interesting bit of information from the lengthy FDA release is their estimate of vaccine efficacy for older age groups.
The numbers are…bleak:
Observed estimates of vaccine effectiveness against symptomatic disease due to the Omicron variant include the following: 8.8% (95% CI, 7.0 to 10.5) at 25 or more weeks since primary vaccination in adults; 59.5% among adolescents 12 to 15 years of age 2 to 4 weeks after dose 2, 16.6% during month 2 after the second dose, and 9.6% during month 3 after the second dose
8.8% effectiveness against symptomatic illness after ~6 months amongst adults.
Within just two months of vaccination, effectiveness against symptomatic illness amongst 12 to 15 year olds drops to 16.6%, and 9.6% by the third month. They don’t specify effectiveness afterwards, presumably because it drops to zero percent or even turns negative.
Furthermore, their estimates of vaccine effectiveness against hospitalizations and emergency department visits are dramatically lower than the 95-100% rates claimed by “experts” that were used to justify discrimination and horrifying calls to exclude the “unvaccinated” from medical care:
Observed estimates of primary series mRNA vaccine effectiveness against hospitalizations due to the Omicron variant in adults have been reported at 41%-57% at 6-9 months or longer after the second dose.
In one observational study among adolescents 12 to 18 years of age (median interval since vaccination, 162 days) during the Omicron-predominant period, primary series vaccine effectiveness was 40% (95% CI, 9 to 60) against hospitalization for COVID-19
Observed estimates of primary series mRNA vaccine effectiveness against emergency department/urgent care visits due to the Omicron variant in adults have been reported between 31%-38% at 6-9 months or longer after the second dose.
Whatever the claimed efficacy percentage was pre-Omicron, these percentages are greatly diminished compared to expectations.
As low as 41% for vaccine efficacy against hospitalization for adults 6-9 months or longer after the second dose.
Emergency department or urgent care as low as 31%. 40% with a confidence interval of 9-60% for adolescents 12-18 years of age.
This is yet another reason why mandates based on vaccination are completely indefensible:
These numbers are remarkably low and would fail the original 50% target that the FDA set for emergency authorization of COVID vaccines.
Remember the concerning part I mentioned earlier about the process for young kids?
Not only are the effectiveness percentages not reaching their 50% threshold in adults, for kids, they simply threw out that standard.
In order to authorize the vaccine for younger age groups, the FDA imputed vaccine efficacy by “immunobridging” and comparing antibody generation from older age groups:
Vaccine effectiveness was inferred by immunobridging based on a comparison of immunogenicity endpoints (SARS-CoV-2 neutralizing antibody geometric mean concentrations (GMTs) and seroresponse rates 1 month after Dose 3) between participants 6-23 months of age from study C4591007 (n=146) and participants 16 through 25 years of age from study C4591001
Essentially, even though antibody creation is clearly not enough to prevent symptomatic infection, or achieve the original 95% estimates, the FDA inferred effectiveness of vaccination amongst babies and toddlers based on comparisons of antibody generation.
At this point, it’s already obvious why the U.S. is going to be the only Western country to start mRNA vaccinations for children this young.
Political pressure from Acting President Klain, activists like Ashish Jha, Jeremy Faust, Jerome Adams and others is undeniably dangerous.
This might potentially explain why the FDA changed the goal from 50% efficacy to antibody generation — to submit to political pressure from the White House and their allies in the media and “expert” community.
Last month, Vinay Prasad detailed the absurdity of this decision:
He also mentions that the 50% target initially determined was “arbitrary” and quite low.
The effectiveness of the vaccinations against hospitalization during the Omicron era for those who are “fully vaccinated” is lower than that, and they inferred efficacy amongst young kids based on antibody generation in those same age groups.
In short, they threw out their arbitrarily determined target, which was already low, and then imputed efficacy based on an end point (antibody generation) that we’ve already seen does not work particularly well against the current dominant variant.
So sure, this is extremely disconcerting and frustrating, but hey, at least Ron Klain is happy.
Natural Immunity
The FDA in their infinite wisdom also ignored that the CDC’s own estimates, which state that 75% of kids have already had COVID:
Of course, no one involved in this decision making process is willing to acknowledge that 75% of kids were infected with COVID despite masking, school closures and other “interventions” designed to prevent or “slow” the spread of the virus. But I digress.
Natural immunity is likely more protective against future infection than vaccination, as this Tracy Høeg tweet explains based on data from a New England Journal of Medicine study:
The FDA raced to authorize the vaccines for extremely young children based on antibody response instead of efficacy estimates while ignoring that 75% of young kids already had better protection.
It’s a clinic in what not to do.
Actual Efficacy Estimates
The FDA did generate some vaccine efficacy estimates for both ages 6-23 months and 2-4 years and the figures they arrived at show why they had to resort to antibody response instead of actual proven reduction.
Participants 6-23 months of age
A preliminary descriptive efficacy analysis of COVID-19 cases occurring at least 7 days post- Dose 3 among participants 6-23 months of age in the Dose 3 evaluable efficacy population included a total of 3 confirmed cases accrued in participants with and without evidence of prior SARS-CoV-2 infection up to the data cutoff of April 29, 2022. The Dose 3 evaluable efficacy population included 376 participants randomized to BNT162b2 and 179 participants randomized to placebo. The VE estimate in this preliminary analysis was 75.6% (95% CI: -369.1%, 99.6%), with 1 COVID-19 case in the BNT162b2 group compared to 2 in the placebo group (2:1 randomization BNT162b2 to placebo).
Emphasis Added
There was 1 case in the vaccination group and 2 in the placebo group. That’s it.
That’s how you get to confidence intervals of -369.1% to 99.6%. The vaccine could have nearly 400% negative efficacy for babies, or it could be one of the greatest vaccines ever created with near perfect effectiveness. Who knows! Certainly not the FDA based on 3 total cases of COVID in this age group.
But don’t worry, they collected a lot more data for the 2-4 year age group.
That data set had 7 total cases:
Participants 2-4 years of age
A preliminary descriptive efficacy analysis of COVID-19 cases occurring at least 7 days post- Dose 3 among participants 2-4 years of age in the Dose 3 evaluable efficacy population included a total of 7 confirmed cases accrued in participants with or without evidence of prior
SARS-CoV-2 infection up to the data cutoff of April 29, 2022. The Dose 3 evaluable efficacy population with and without evidence of prior SARS CoV-2 infection included 589 participants randomized to BNT162b2 and 271 participants randomized to placebo. The VE estimate in this preliminary analysis was 82.4% (95% CI: -7.6%, 98.3%), with 2 COVID-19 cases in the BNT162b2 group compared to 5 in the placebo group (2:1 randomization BNT162b2 to placebo). One confirmed case in the placebo group occurred in a participant with evidence of SARS-CoV-2 infection prior to 7 days post-Dose 3.
Well at least we’re down to a possible 8% negative efficacy in the confidence intervals!
But again, don’t worry, the FDA is aware of this limitation, and many more besides:
In a combined analysis of both age groups, VE was 80.4% (95% CI: 14.1%, 96.7%) with 3 cases in the BNT162b2 group and 7 cases in the placebo group. Interpretation of post-Dose 3 efficacy data for both age groups, and for the age group of 6 months through 4 years overall, is limited for the following reasons:
- Vaccine efficacy post Dose 3 cannot be precisely estimated due to the limited number of cases accrued during blinded follow-up, as reflected in the wide confidence intervals associated with the estimates.
- These descriptive efficacy data are preliminary, as the protocol specified 21 cases have not yet been achieved.
- There were highly variable dosing intervals between doses 2 and 3, with median intervals of 112 (range 56 to 245) days among participants 6-23 months of age and 77 (range 42 to 239) days among participants 2-4 years of age in the Dose 3 evaluable efficacy population.
- The median blinded follow-up time post Dose 3 in the analyses was only 35 days for participants 6-23 months of age and 40 days for participants 2-4 years of age.
The protocol specified 21 cases were not achieved. But they authorized the vaccines anyway!
Amongst the 2-4 year age group, there was a significantly higher rate of cases that “met the criteria for severe COVID-19” in the group that received the vaccine:
Seven cases in participants 2-4 years of age met the criteria for severe COVID-19: 6 in the BNT162b2 group, of which 2 cases occurred post unblinding, and 1 in the placebo group.
This does not imply that those who get vaccinated are more likely to have a severe case of COVID, but it once again underscores the problem of such small sample sizes and abandoning the original targets.
And it should be noted that the severe cases were determined to not be “clinically significant:”
All of which were considered by the investigator as not clinically significant based on examination at the illness visit and contributing circumstances such as the participant crying during examination
The Data Tables
The FDA knows that most Americans will never look at the data tables, especially those in the media and activist Twitter “expert” class.
But anyone who does examine them can immediately understand the absurdity of the FDA’s decision making process:
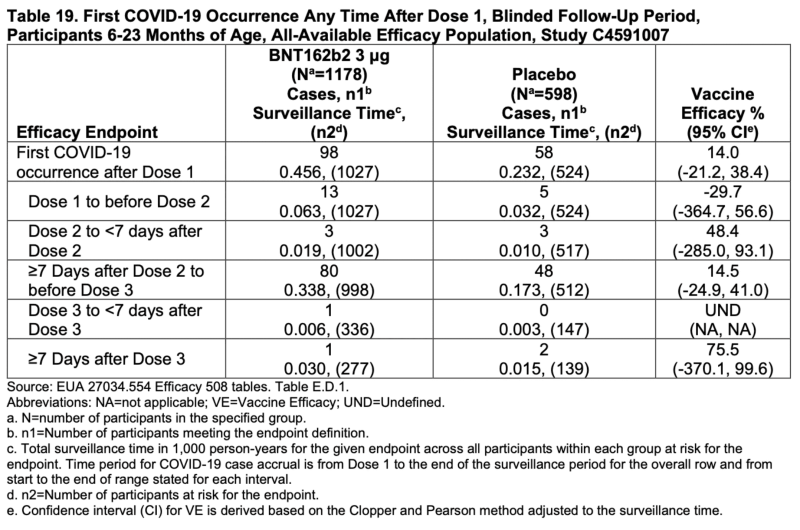
The confidence intervals for every single efficacy calculation for participants 6-23 months drop below zero. Every single one.
The overall estimate is 14% and even that could be as low as -21.2%.
It’s just laughable. Well, it would be laughable if it weren’t such an important decision.
If you want to be charitable, at least the overall efficacy percentage for those aged 2 to <5 didn’t have negative confidence intervals:
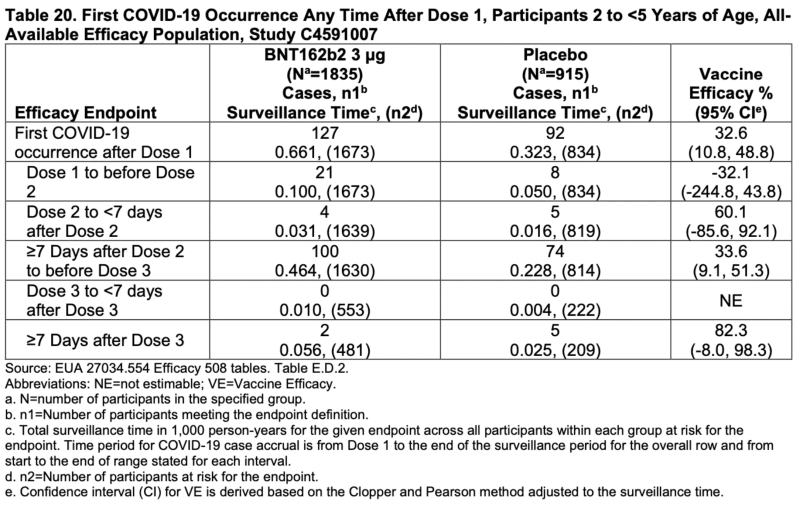
Although three of the four main endpoints did have negative confidence intervals, so it does still require a significant amount of charity.
It’s also worth noting that the time period between the administration of Dose 1 and Dose 2 was associated with negative efficacy in both age groups.
This has likely contributed to data reporting issues when calculating vaccine effectiveness in the real world. Any case occurring during this time period is considered “unvaccinated,” except in these age groups, which is when efficacy is at its lowest point.
The fact that the FDA authorized these vaccines for kids based on this data is quite simply inexcusable.
The sample sizes didn’t meet their protocol specified 21 cases.
Vaccine efficacy calculations, even excluding the gigantic confidence intervals, were far below the arbitrary 50% target they created for emergency use authorization among adults.
Including the confidence intervals shows the possibility of negative efficacy, which while unlikely, is still possible given the extraordinarily small amount of cases in both the vaccine and placebo groups.
They simply used “immunobridging” to infer protection based on antibody generation, instead of predetermined efficacy rates.
It’s yet another terrifying indicator of just how politically motivated the FDA has become, and how activism has distorted intellectual honesty.
“Experts” are so desperate to maintain their reputations and avoid being labeled an “anti-vaxxer” by influencers like Eric Feigl-Ding, Angela Rasmussen and others that they appear to be unwilling to call out flaws in the decision making process.
It’s simultaneously hard and easy to believe that this was all it took to justify an “emergency” use vaccination for age groups at extremely low risk of severe illness.
This decision deservedly will be yet another reason for the ever-increasing erosion of trust in public health’s supposed “experts,” an embarrassment for U.S. regulators captured by politics.
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








