
We all make the mistake of thinking “Americans” have the same culture, the same beliefs & values. However, while united in our democratic experiment and the pot of money into which we pay our federal taxes, we Americans are a diverse, pluralistic people spanning a vast range of religious, socioeconomic, racial, political, and other beliefs and circumstances.
Our built environments range from metropolitan wonders of the world like New York City to remote outposts of Innuit villages in Alaska. Our homes range from massive mansions and towering skyscrapers to homes on the prairie, rustic lodges, and desert hogans without running water. Many Americans are liberated from organized religion and free to roam the world as agnostic or atheistic, and others are devoutly religious members of organized religion who believe in eternal damnation, reincarnation, and more. We have cities advancing the technological frontier with 5G networks and iPhones in every pocket, and we have the Amish.

In our large and diverse country, a failure to apply standard public health practices of cultural relativism and appreciate American pluralism when conceiving public health policy can – and almost surely will – result in an overreliance on ethnocentric policy recommendations, such as contact tracing apps that clearly underserve the Amish. Ethnocentric public health policy is unethical – it can underserve groups of people underrepresented in science, and it can undermine public health.
Our national and international public health policy is vulnerable to ethnocentric policy recommendations because science, like many sectors of our economy, has a diversity problem. While 18.4% of Americans are Hispanic, only 8.4% of epidemiologists are Hispanic; while 13.4% of Americans are black, only 5.4% of epidemiologists are black. While 23% of Americans are Republican, only 6% of scientists are Republican. I have yet to meet an Amish scientist, but perhaps that’s because most scientific work occurs online.
While contact tracing apps for the Amish are obviously ridiculous, there are other, far more harmful examples of ethnocentrism in science and policy disagreements in COVID-19. One particularly potent example of ethnocentrism in COVID-19 policy is the way scientists dismissed conservative policies in the contentious debate between the mitigation of viral harms through focused protection, and the containment of the virus through society-wide changes like lockdowns, travel and trade restrictions, and school closures.
Containment versus Mitigation
Containment and mitigation, the things we’ve been arguing about for over two years, are a false dichotomy of pandemic control. Yet, we argued this dichotomy and any historian trying to understand what happened during COVID has to understand the context of “containment” policies as opposed to “mitigation” policies.
Controlling a virus is done through a mix of reducing the viruses’ severity and decreasing viral transmission. We can reduce severity through treatments, we can reduce transmission through various behavioral changes and non-pharmaceutical interventions, and we can reduce both transmission and sometimes severity through vaccinations. The challenge with COVID-19 was that we had little in the way of proven safe, effective, and widely available treatments, and phase 3 trials for vaccines were not completed until late 2020.
For the entire year of 2020, we had no vaccines and the scientific questions centered on how bad COVID-19 would be if it ripped through a population without any mitigation, how much mitigation could reduce COVID-19 hospitalizations and mortality, and what collateral damage could our non-pharmaceutical interventions cause. Building on the foundations of those unanswered scientific questions were pandemic public health policies, and the central policy question we faced in 2020 was how far we were willing to go to reduce transmission in a gamble for vaccines.
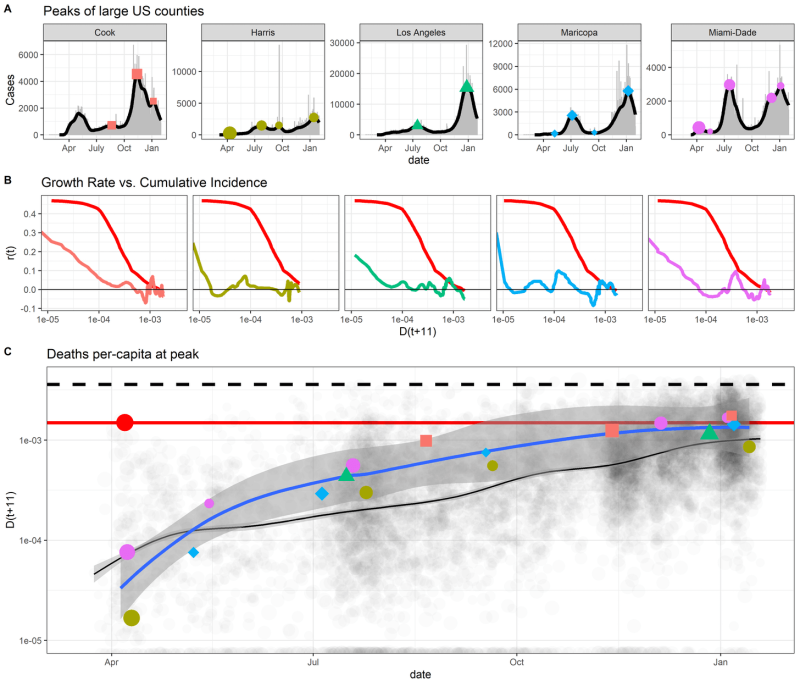
Containment proponents were willing to go the farthest to reduce transmission, all in a large gamble that vaccines might prove safe and effective and save more lives than would be lost from collateral damage from stringent COVID policies. Containment advocates believed that COVID mitigation efforts would result in 0.4% of the population in a US county or state dying for cases to peak, with up to 0.5-0.8% of the population dying by the end of the pandemic wave. For containment proponents, it was reasonable to force people to stay in their homes, to close schools, to restrict travel & trade, to do anything possible to stop the virus and wait for a vaccine, otherwise millions of Americans would die.

Containment proponents also tended to avoid talking about the costs of their policy proposals but would propose to alleviate the harms caused by pandemic policies by increases in federal spending to subsidize labor. Containment proponents imagined a federal government skilled and capable of tending to the diverse needs of Americans disrupted by unprecedented policies.
Almost none had solutions for how to alleviate the harm our national actions caused to people outside our borders, such as the surge in >20 million people facing acute hunger predominately in Africa and Asia or >100 million kids worldwide facing multidimensional poverty as a result of economic contractions from lockdowns, travel & trade restrictions, and widespread fear of a virus, we were told, could kill 0.6-1% of the people it infects.
Mitigation proponents, on the other hand, believed the estimates of COVID pandemic burden were highly uncertain or overestimates, that the estimated public health costs of pandemic policies were too low and real human and public health costs of containment policies may be higher, that the federal government may not be sufficiently nimble to meet the diverse needs of 340 million people whose lives were disrupted by outbreak control policies, and that harming people in the service of public health is unethical. They proposed abandoning the vaccine gamble and instead focus efforts on protecting patients at high risk of severe COVID-19 without requiring we reduce transmission to zero.
Mitigation proponents focused on protecting nursing homes, allocating tests & N95 masks to care facilities that accounted for nearly 50% of the deaths in early COVID-10 outbreaks. Instead of subsidizing labor for hundreds of millions of Americans with stimulus checks that could cause inflation, and having no plan for dealing with hunger and poverty outside our borders, mitigation proponents argued for a relaxation of restrictions and providing focused economic support for a few million people who are at high risk of hospitalization or death from COVID-19.
In mid 2020, while epidemiologists warned about the harms of the virus, economists were warning of the harms from our responses to the virus. Signs of supply chain disruptions were emerging due to lockdowns, travel/trade restrictions, and changes in consumer behavior from messages of a highly severe pandemic combined to increase poverty and acute hunger, as people living on $1 a day no longer made $1 a day, while also disrupting the transportation networks used by humanitarian organizations to stave off starvation in the world’s poorest people.

The Great (Barrington) Debates
As noted, “Containment” versus “Mitigation” is a false dichotomy of disease control. However, a great deal of American deliberation of pandemic policy devolved into a tribal discussion of “Containment” versus “Mitigation”, with clear partisan assortment into camps as mainstream epidemiologists and liberals called for stronger federal and international disease control while many economists, conservatives, and some epidemiologists called for mitigation approaches that reduce collateral damage from COVID-1 policies.
Scientists varied in their estimates of SARS-CoV-2 severity, the health and economic costs of pandemic policies, and the probable efficacy of various non-pharmaceutical interventions. Yet, despite these legitimate disagreements among scientists on the scientific foundations of pandemic policy, many scientists failed to acknowledge these legitimate disagreements, and many major institutional public health figures largely embraced containment policies and messaging while creating straw men out of mitigation arguments.
On October 4th, the Great Barrington Declaration was signed & released to the public, advocating for focused protection as a public health policy capable of reducing the harm of the pandemic and public health policies.
On October 8th, 2020, the head of NIH Francis Collins and the head of NIAID and US pandemic policy figurehead Anthony Fauci emailed one-another calling for a “devastating take-down” of the Great Barrington Declaration. While “herd immunity” is not mentioned anywhere in the Great Barrington Declaration, many containment proponents began misrepresenting focused protection as a “herd immunity” strategy.
On October 12th, 2020, the WHO Director-General called mitigation a “herd immunity strategy” and argued that ‘never in the history of public health has herd immunity been used as a strategy’. On October 14th, Rochelle Walensky (who now runs the CDC), Marc Lipsitch (Harvard T-Chan epidemiologist who now runs the center for outbreak forecasting & analytics at the CDC), Gregg Gonsalves (public health professor at Yale commonly lambasting the GBD on Twitter, who also goaded Fauci to step up the federal response to COVID-19 in March 2020) and Carlos del Rio wrote an article condemning the Great Barrington Declaration as a “herd immunity strategy”. Marc Lipsitch had consulted Pfizer and Moderna on their COVID-19 vaccines, a conflict of interest not declared on the Washington Post article arguing millions of Americans could die unless we stop transmission until vaccines arrive.
In the background of the Great Barrington Declaration, however, important scientific evidence was emerging. From the beginning of the pandemic, Sweden had adopted mitigation polices for COVID-19 and chose to refrain from closing schools, bars and restaurants to focus their protection on patients at high risk of severe COVID. For this transgression, Sweden was demonized by the scientific and public health policy messengers in mainstream US media outlets. Of note, Martin Kulldorf, one of the co-signers of the Great Barrington Declaration is from Sweden, yet rather than curiously understand Swedish culture, beliefs and values, and how these cultural differences may underlie Dr. Kulldorf’s alignment with Swedish policy, scientists lambasted both Sweden and the Great Barrington Declaration.
Many US epidemiologists and public health figures became armchair pundits, lobbing political criticisms at Sweden without a deep awareness of Swedish culture, and these same pundits were driving US policy and pandemic media coverage in a manner quite dismissive of legitimate alternative views on both science and policy.
Let’s zoom out a bit to see the big picture.
There was legitimate scientific disagreement on COVID burden and on the costs and benefits of non-pharmaceutical interventions. In a massive, pluralistic country with deep political divisions about the relative roles of state versus federal governments, in which the CDC is a non-regulatory agency and states are granted powers not enumerated in the constitution, a small political monoculture of scientists pulled the reins of our country’s public health policy towards their political preferences, most clearly when Gregg Gonsalves goaded Anthony Fauci into orchestrating a federal response to COVID-19.
The US federal public health policy messaging on COVID-19 mirrored international health organizations like the WHO, which all mirrored the false-consensus presented by mainstream media messaging on COVID-19, all of which encouraged society-wide changes, from lockdowns to bar/restaurant & school closures.
The platter of policy choices presented to Americans by leading epidemiologists was not an exhaustive, objective set of solutions to a scientific problem presented in an unbiased way. Rather, American federal policymakers and a coterie of closely connected epidemiologists prioritized favorable presentation of policy preferences chosen by these scientists driving the epidemiological and public health narrative in America.
Americans differ in their beliefs, norms and values, and while some may value a strong government intervention aimed at stopping a pandemic, others may equally strongly, and with equally legitimate cultures and morals derived from their entire lives spent living in their communities, wish for powers of public health to be left to states and/or the people. We have a government with shared powers between states and a federal government, and considerable disagreement among Americans about who should do what during the pandemic. The critical point here is that both liberals and conservatives are Americans, and we differ sufficiently in our views to warrant a more culturally relativistic treatment in public health.
However, the science presented to Americans, such as estimates of millions of deaths under mitigation policies, was in debate. Built on a biased presentation of scientific uncertainty, figureheads in epidemiology and public health could not impartially present policies aligned with conservative values, nor did they put their minds to the task of maximizing the effectiveness of public health efforts within the constraints of conservative beliefs & values. Containment policies that became “the message” from public health figureheads in America were presented as the objective and morally superior answer to the pandemic, but they were in fact subjective policy preferences from people who disproportionately come from one end of the spectrum of American political beliefs.
Alternative policies such as mitigation presented by the Great Barrington Declaration and adopted in places like Florida and South Dakota sincerely aligned with the beliefs and values of some Americans. However, these alternative policies – which should rightly be viewed as participatory public health from one underrepresented, distinct cultural group in America – were lambasted as unethical, immoral, murderous, “genocidal” and “eugenicist” (I wish I was joking) by members of another cultural group in America.
When the rare beacons of political and scientific diversity in the field voiced their disagreements with this false consensus on science and policy, the heads of NIH and NIAID orchestrated a devastating take-down. Within 10 days of proposing to “orchestrate a devastating take-down” of alternative public health policy proposals, we saw exactly what Collins and Fauci desired.
A public health call similar to “won’t someone rid me of this meddlesome fringe?” was followed by a flurry of hit-pieces coming from every corner of our information ecosystem, including blue check-marked Twitter profiles stamped as official, credible sources of information to editorials from famous epidemiologists in mainstream outlets like Washington Post, and even the WHO director general. The hit pieces are viewed by their supporters as necessary to maintain unity in public health messaging, but they can also fairly be viewed as cross-cultural conflict in which one culture – liberals – had greater access to institutional public health power, from epidemiological prestige and media connections to official appointments at the head of our federal government.
A conflict theorist’s view of COVID-19 containment versus mitigation debates can rightfully view that scientists, themselves immersed in cross-cultural conflict, used their institutional power to make conservatives’ – the other culture’s – preferred policies look stupid, unethical, and scientifically wrong. It is not within the rulebook of ethical public health policy to weaponize the privileged authority granted to scientists and public health leaders in order to suppress engagement and participation of minority cultures in the public health process.
The intention of this flurry of political hostility towards the Great Barrington Declaration specifically, and towards mitigation polices & their proponents more broadly, was to reinforce a message that mitigation policies would result in millions of Americans dead, that vaccines were necessary to save millions of American lives, and that Americans should support policies like shelter-in-place orders, school closures, vaccine mandates, that Brits should support a nationally orchestrated whack-a-mole game of tiered lockdowns, and countries with a long history of promoting civil rights should tolerate violations of civil liberties despite protests and a lack of informed consent from subcultures in our pluralistic society. Furthermore, some involved in this messaging had either consulted vaccine companies positioned to make billions of dollars off of this gamble, or assisted Operation Warp Speed and, consequently, massive conflicts of interests were undisclosed or undiscussed.
The perils of public health monism
As mentioned above, the common defense of the blitzkrieg against the Great Barrington Declaration, and against scientists like Levitt, Ioannidis and others who spoke out earlier, was that these rogue scientists, by speaking their sincerely held views, were introducing conflicting messages, and conflicting health messages can produce adverse outcomes. If scientists estimated – however sincerely – that SARS-CoV-2 might not kill 1% of the people it infects but, rather, might kill 0.2-0.4% of the people it infects, then, it was argued, such estimates might trigger risk compensation and complacency that increases the number of people who die from COVID.
While conflicting health information can sow confusion and can lead to adverse outcomes, it’s also true that presenting a false consensus on scientific issues gambles public health’s credibility on uncertain science and, should the gamble go wrong, can sow widespread distrust in scientists and public health officials precisely when trust is needed. It’s also true that ethnocentric public health efforts can cause harm by proposing policies ill-fitted to people.
We talk about ethnocentrism in public health when advising Europeans and Americans on how to approach doing public health in places like Africa, but these anthropological principles still apply when working in our own country. It’s ethnocentric for liberals who have spent most of their lives in the NE corridor to project their culture, beliefs and values to think their preferred policies are the most appropriate public health policies for conservatives who spent most of their lives in rural South Dakota.
The science is out, and the estimates of pandemic burden provided by containment proponents were, in fact, massive overestimates. South Dakota, Florida, and Sweden became the world’s control groups – these regions rejected costly containment policies in favor of focused protection polices. Yet, in mid-October 2020, the world’s leading epidemiologists and public health policy messengers claimed 0.4% of the population would die just for cases to peak, but in all of these regions following mitigation policies, cases peaked when 0.1% of the population died, with much more time left over for seasonal forcing to drive cases higher, yet cases declined without vaccines.
Many people died from COVID, but containment proponents estimated that for every person that died in the saturated hospitals of South Dakota, three more would have died in their homes, and those estimates were used to justify strong federal responses to COVID-19, devastating takedowns of different – smart and legitimate – policy perspectives, and other acts of hostile intolerance that limited the diversity of science & public health policy. That doomsday scenario never came to pass, and that doomsday scenario was cornerstone to containment policies.
Beyond the false consensus undermining the science of epidemiology itself, the public health policy monism around containment strategies presented by mainstream epidemiologists and public health figures was not the only approach to public health policy in America, it was a reflection of the limited political diversity of this group. By improperly using their scientific authority and positions in federal bureaucracies to invalidate conservative participatory efforts in public health, these mainstream epidemiologists and public health experts acted in a manner that was egregiously, historically ethnocentric.
It’s no surprise that liberals in this pluralistic country would want a stronger federal messenger for COVID-19 policy, as Dr. Gregg Gonsalves did when he reached out to Fauci in March 19th 2020 urging for stronger federal messaging. Liberals in the United States love delegating tasks to the federal government, liberals trust the federal government (especially appointees in executive agencies like NIAID), and they have a vivid imagination of what a nimble, sophisticated, and highly skilled federal government is capable of. Liberals’ relationship with the federal government stands in stark contrast to conservatives’ views of the federal government as an oversized, bureaucratic monster creating clumsy inefficiencies.
Conservatives may better trust local messengers and local policies, and many of those local policies may prioritize the right over the good, or they may balance competing risks of COVID and other causes of death, including deaths outside the US such as the >20 million people who faced acute hunger in Africa and Asia as a result of containment policies and widespread fear of COVID.
Many epidemiologists, however, utilized their privileged positions as professors at elite institutions, and their connections to Anthony Fauci and major media outlets to pull US policy in liberals’ preferred direction. The ethnocentric imposition of their policies onto a large and pluralistic country came at the expense of the country’s conservatives, among others grossly underrepresented in science, whose beliefs, norms and values were not fairly represented in the American public health process during COVID. When diverse political values manifested in diverse policies across Florida, Texas, and South Dakota, the governors of these states became targets of waves of online hostility from scientists and public health experts, and epidemiologists labelled their activities as immoral.

For a second, let’s imagine all of the epidemiologists and public health figures were American and British, and instead of discussing public health policy of Florida, Texas, and South Dakota, the regions proposing different policies were concentrated in Latin America and low-income countries in Africa. Most in contemporary public health agree it would be unethical for a small contingent of predominately White Western epidemiologists to overestimate the severity of a disease, sow fear in these countries full of people with different cultures, and use their larger media reach to push their preferred public health policy agenda onto other people & cultures. Yet, somehow this naked ethnocentrism is undiscussed, and in fact is argued to be ethical when done entirely across cultures within America.
It would not be unethical to push one’s policies if Americans are all the same culture and/or if it were objectively clear when culturally relativism is supporting participation in public health policy versus when ethnocentric policies are imperialistic impositions weaponizing an imbalance of power. Of course, Americans are vastly multicultural and the public health norm against ethnocentrism, of valuing participation, is not objectively clear but rather socially constructed, and so we have to ask ourselves: do we really believe in the purported principles of encouraging participation in a pluralistic world? When do these rules no longer apply? Was it ethical for leading epidemiologists and public health figures to use their imbalance of power to demonize conservative participation in public health during COVID-19?
The treatment of conservative policies by scientists and public health officials of in COVID-19 was nakedly ethnocentric, a tragic reflection of a field lacking political diversity and consequently trapped in a self-reinforcing ideological bubble. It’s hard to imagine many young conservatives would want to become an epidemiologist after this experience in COVID, and in fact this cultural monism is part of the reason why I left epidemiology.
I grew up in New Mexico with many Libertarian friends, with a family farm lacking potable running water like many of the homes in nearby Navajo Nation, and I found the lack of cultural and political diversity of epidemiology blinded the field and its leading voices of legitimate cultural differences in America. The naked ethnocentrism and political intolerance of prominent epidemiologists during COVID excluded diverse voices from the discussion in favor of supporting a false consensus in science, and an unethical monism of public health policy derived from the exclusion of many American sub-cultures from the public health process.
The fields of epidemiology and public health purport – by their own social construct – to have ethical obligations to avoid ethnocentric policy when working in Africa and Asia. Mots public health scholars learn historical examples of how ethnocentric public health policies by White scientists caused harm to people of color in different cultures. However, that same principle of tolerance for anthropological variation, the insistence on cultural relativism, was thrown out the window when it came to dealing with our fellow Americans.
Epidemiology and public health, with such profound underrepresentation of conservatives in our ranks, united around an intolerant monism of policies that did not reflect the beliefs and values of conservatives, and other cultures in our pluralistic society. When conservatives proposed mitigation policies they would support, epidemiologists weaponized their expertise and media connections derived from their positions as ethical scientists to delegitimize these fair, pluralistic views.
Within the scientific community the Great Barrington Declaration was falsely criticized for being funded by a libertarian think tank – the think tank was not libertarian and did not fund the GBD – yet a culturally relativistic anthropologist would acknowledge that libertarianism is not a bad word, it is a political philosophy held by 17-23% of the American electorate and held by almost no scientists, and the scientific community’s demonization of political philosophies held deeply by many Americans, but not by scientists, is a damning example of poor diversity in the sciences yielding ethnocentric public health policy in a national emergency.
To put it simply, conservatives are people, too. Epidemiologists and public health scholars need to reexamine their anthropological ethics to clarify why conservatives in America were not given the same humanizing benefit of the doubt during COVID as non-White cultures are given in other public health responses around the world. It would be wrong to say conservatism is not a culture worthy of equal treatment, protection, and humanization by public health. A broader appreciation for and tolerance of cultural differences in our pluralistic society would humanize our anthropological variation and invite different cultures to participate in the public health process regardless of whether these cultural differences occur along racial, religious, regional, socioeconomic, gender, sexual, or political axes of human variation.
The literature trail of scientists attacking conservatives is long. The political and partisan hostility wielded by public health scholars in a time of crisis underserved vast swaths of Americans with different beliefs, norms & values who are underrepresented in science, who are sincerely conservative or libertarian, and these scholars created a culture hostile to the few conservatives in epidemiology and public health at precisely the time when we needed diversity, representation, participation, engagement, and all hands on deck. These same public health scholars who demonize conservatives in America went to great extents to drive the American federal public health response to COVID-19.
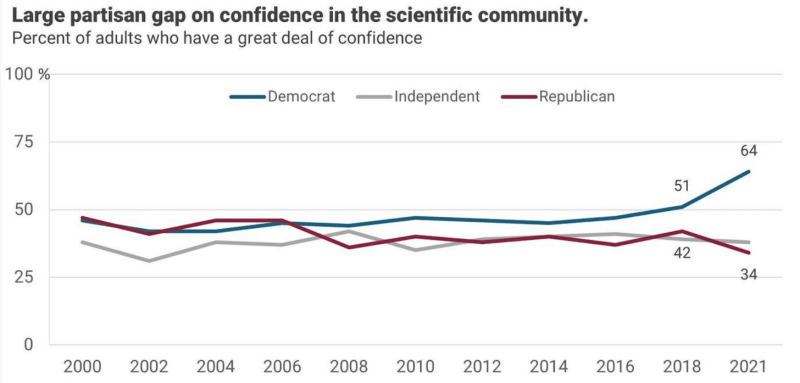
Now, there are more COVID-19 deaths in red counties than blue counties, an effect largely attributable to lagging vaccine uptake in red counties prior to the Delta wave. As we stare down this unusual social/political determinant of mortality during COVID, an unsettling question we have to consider is that perhaps scientists failed conservatives. Conservatives and others proposing mitigation policies were telling us what they would prefer to do, they were participating in public health. However, because conservatives’ values and preferences differed from those of most epidemiologists, epidemiologists demonized conservative policy proposals, and conservatives began to rapidly distrust science while liberal trust in science skyrocketed.
With the same seriousness we look at racial and social inequities in health, we have to examine these political inequities in COVID-19 mortality, and this partisan divergence in trust in science, and ask: did epidemiologists impartially serve all Americans during COVID? Could these inequities have been reduced if epidemiologists and public health officials had more compassionately, and less ethnocentrically, embraced American pluralism in public health policy?
Did Blue epidemiologists underserve Red America?
American pluralism in public health policy
I’ve focused on conservatives here because I have a few conservative bones in my body and can speak from experience. Conservatives are clearly an underrepresented group among epidemiologists and public health officials, and conservative beliefs and values differ sufficiently from liberal beliefs & values to justify sincerely desired yet very different public health policies.
Conservatives are not historically marginalized in the same way racial minorities, commonly the subjects of “cultural relativism”, were. Yet, by being culturally distinct, by being so underrepresented in science, and by comprising a large share of people and even representatives in our polarized democratic republic, conservatives test our commitment to ideals of tolerance in science and our public health ethics warning against the harms of underrepresentation from non-inclusive work environments, and ethnocentrism in science and public health policy.
In the case of COVID, it was Conservative policies that were notoriously ridiculed by the dominant, disproportionately liberal political culture of epidemiologists and public health officials, and conservative think tanks’ propositions for policy responses to COVID were seen as corrupt or evil by many scientists with preconceived animosity for conservative groups.
From one angle, scientists may see themselves as holding back a tide of misinformation and safeguarding message clarity in public health policy, but from another angle scientists in COVID may be fairly seen as being openly hostile towards, and thereby underserving, an underrepresented group in science during a time of deep partisan rifts and widening cultural speciation within America.
In our fiercely partisan times, is it even possible for scientists and public health experts, with their overrepresentation of one of two parties, to serve as impartial, unconflicted guides of their own country? Or do the political biases of scientists tilt the scales of policy and favor the scientific evidence supporting whichever party has more scientists?
We ask the same questions of race, of whether white justices are capable of objectivity in cases involving race. We ask the same questions of sex and gender, whether men on the Supreme Court can handle cases involving women’s rights objectively, whether straight justices can understand and remain objective on queer rights. It’s only fair, and in the interest of liberalism’s goal of tolerant pluralism, to ask the same questions of whether scientists in a polarized public are capable of objectivity despite their biased political composition.
The broader goal of embracing American pluralism is much larger than inspiring scientific tolerance across our partisan divides. The full scope of American pluralism covers spectra of race, region, socioeconomics, gender, religion, etc., and how all of these intersect. Yet, in public health there is a common ethical standard of cultural relativism, an ethic thrown out the window during COVID-19 when liberal scientists demonized conservative participatory efforts. Before the next pandemic, we must reinforce the ethical pillar of cultural relativism in public health with a fresh look at America’s many cultures and an unsparing debrief of which major subcultures were not adequately represented or tended to by epidemiologists or public health officials.
The Way Forward
The first thing we have to realize is that one size rarely fits all across our large country. While tech employees in New York City can work from home instead of riding the subway to work every day, people working oil rigs in Texas, ranches in Montana, and farms in Iowa may not be able to work from home. While many white people live in small homes with their nuclear families and can separate themselves from the grandparents, many Hispanic and Native American people live in large multigenerational homes with essential workers, and elders are the primary caretakers of kids and in these multigenerational homes protecting the elders may benefit from specific kinds of support, from more deliberate action, more focused protection.
Across our vast, heterogenous human populations of the US, a policy or a public health message that works where you live may very well harm people who live somewhere else, who have different cultures, beliefs and values. As one size may never fit all, it becomes increasingly important for scientists helping a pluralistic world to avoid political monism at all costs, to deliberately create space for alternative ideas.
Second, we have to appreciate our own limited positionality and ender rooms with a great deal of humility about what polices or messages might work for people from other cultures. Many predominately white epidemiologists living in the NE corridor said that “focused protection” and protecting the elderly could never work. In their communities and cultures, the elderly are exposed to the virus everywhere in dense metro areas, in buildings and on subway trains. However, in Native American tribes across the west, elders are identifiable and revered members of the tribes and “protect the elders” resonated with tribal culture enough to became a motto behind communal efforts to focus protection from Navajo Nation in New Mexico to Blackfeet Nation in Montana. In my wife’s Hispanic family, we implemented a focused protection approach to safeguarding Abuela, my wife’s elderly grandmother.
Our focused protection prioritized reducing the risk of transmission to Abuela, and additionally utilized the closely connected extended family to set up a program for rotating who is living with Abuela. Instead of demonizing focused protection, if scientists acknowledged their unfamiliarity with other communities and, instead, asked “what are some examples of focused protection that would work for your community?” it’s possible we could’ve created space for Navajo Nation to share their story.
It’s possible we could’ve shared our “Abuela Protocol”, and such a protocol may have proven useful for other closely connected extended Hispanic, Native American, and other families. When scientists step down from pretending to know everything about everyone, we can create space for diversity, for people from other cultures to share their experiences, values, and ideas.
Third, to overcome partisanship of scientists, we need to put more effort into seeing the merits of what other people are trying to say instead of trying to out-debate them. For example, whether or not focused protection works became an acrimonious debate, yet few containment proponents saw the merit that focused protection works at various scales. It provided a heuristic for individuals to prioritize their efforts. It provided households and families in many cultures a rubric for planning and preparing for the pandemic to protect the most vulnerable members of the family.
Had leaders in epidemiology and public health been more tolerant and refrained from “devastating takedowns” of competing views, we could’ve come to acknowledge that mask-wearing in subways and on planes are examples of focused protection, focusing our efforts on the most sensitive scenarios. We focus protection when we reduce HIV transmission by providing needles for drug users as opposed to providing needles for just anyone, and so “focused protection” is central to public health policy as it is simply maximizing the cost-effectiveness of our efforts.
At the national level, we implemented focused protection when we prioritized individuals at risk of severe COVID for vaccination, and focused protection could’ve increased the efficacy of our allocation of tests, allocating more rapid tests to nursing homes as opposed to fewer rapid tests to every person in the country. There is merit to thinking about cost-effectiveness, and many conservatives love thinking about this, yet this merit was lost by scientists who reflexively saw their “opponents” as wrong, and needing to be “taken down”.
That focused protection was controversial, and that the Great Barrington Declaration continues to be demonized by scientists at the time of this writing, is a damning indictment of the intolerance of a false consensus on science and a stubborn, misguided monism of public health policy conceived by an unrepresentative field of scientists. To this day, one wonders if the Great Barrington Declaration’s cardinal offense was not the inaccuracy of its science, which was corroborated, or the feasibility of its policy, which in fact connects the GBD with most public health policies, but rather that the wise words happened to be supported by a libertarian think tank and few (if any) famous epidemiologists are libertarian.
Whatever a scientist’s political beliefs, when trying to guide American policy, one needs to remember that conservatives – and even libertarians – are human beings whose culture, norms & values comes from their entire life’s story. If scientists wish to lead a country in a time of crisis, they need to drop their partisan swords and give all humans the benefit of the doubt regardless of the political party or political philosophy of the think tank, and scientists must retain an open mind as people we may disagree with may simply be from a different communities, cultures, or contexts, and they can have good ideas that work well for their communities, cultures and contexts.
To avoid harmful policy monism in the next pandemic in our pluralistic society, we need to limit federal and international messages to the core science, including the uncertainty and disagreements. Instead of suppressing scientific uncertainty and disagreements in a culture of hostility for dissident scientists, we need to allow scientists to make their arguments without fears of persecution for their dissent from an intolerant monoculture.
Rather than pretend the next generation’s Fauci and Collins and Birx and Gonsalves can conceive the right policies for hundreds of millions of people across a vast range of human experiences in our country, we need to create a platform for pluralism that facilitates policy + idea-sharing among people at many scales from households and businesses to counties and state, allowing others to search the aisles of policies across the US for ideas that work for them.
Finally, we need to train epidemiologists and public health officials to have greater awareness of positionality and to exhibit greater cultural humility when acting as scientists and public health leaders in a pandemic. When we enter into communities with fierce partisan rifts, especially when that community is one we grew up in and in which we have our own strongly held partisan beliefs, it is essential we leave our partisanship at the door and serve our roles as scientists and public health leaders in the most impartial way possible to leave no community underserved.
Join the Conversation
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








