New COVID-19 guidance issued by the Centers for Disease Control and Prevention (CDC) may seem like the beginning of a welcomed end to a two-and-a-half-year-old pandemic, but an overreliance on the CDC’s broken and discriminatory Community Level tool may lead to unnecessarily prolonging the pandemic and keeping Americans in masks for years to come.
Based on the improved phase of the COVID-19 pandemic and the widespread availability of several COVID-19 vaccines and treatments, the CDC on Aug. 11 issued loosened guidance. At the same time, however, the CDC’s push to get more government agencies, businesses and schools to adopt its COVID-19 Community Level tool for masking decisions is concerning, because the tool doesn’t factor in the widespread availability of vaccines and treatments when determining levels within counties across America.
What is the CDC’s COVID-19 Community Level tool?
According to the CDC, the COVID-19 Community Level tool helps individuals and communities decide which prevention actions to take based on the latest information. Each level conveys how much COVID-19 is impacting a community using data on hospitalizations and cases. Using these data, communities are classified as low, medium or high.
The Community Level tool does not take into account the following:
- Widespread availability of multiple COVID-19 vaccines and treatments
- County-level vaccination and booster rates
- Decreases in strength of variants and subvariants, hospitalizations and deaths
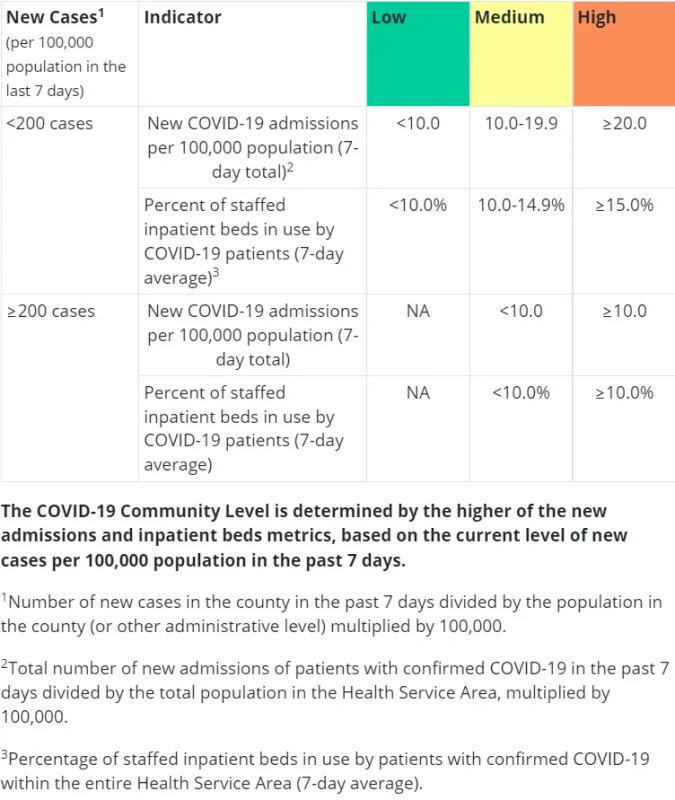
A county’s COVID-19 Community Level is determined by the higher of the new admissions and inpatient beds metrics, based on the current level of new cases per 100,000 population in the past 7 days.
Verifying any of the data used to determine a county’s Community Level is almost impossible. However, in one North Carolina county, an interesting analysis was conducted, thanks to transparency by a local health department.
Dare County, N.C.
The majority of Dare County is located on barrier islands popularly known as the Outer Banks of N.C. Home to three national park units, Dare County receives millions of visitors each year. It also has a health department that shines when it comes to transparency. Every Monday, the Dare County Department of Health and Human Services (DCDHHS) publishes on its website the number of COVID-19 cases, hospitalizations and deaths over the past seven-day period. Local data are the most accurate data, according to the CDC.
Due to consistent reporting by the DCDHSS, Dare County, N.C. was chosen as a data analysis location for nine weeks, between June 9 and Aug. 4, 2022.
The first observation made was that the COVID-19 cases reported by DCDHHS never matched up with the N.C. Department of Health and Human Services (NCDHHS) reporting of cases for Dare County and the NCDHHS numbers never matched up with the CDC’s reporting of cases for Dare County. It is especially odd that the NCDHHS numbers didn’t match the CDC’s numbers for Dare County because the CDC’s Surveillance Review and Response Group stated in an email exchange that “case and hospitalization data are sourced directly from the NCDHHS.” If the case numbers never matched in nine straight weeks, where are the case numbers coming from?
Even though Dare County receives millions of visitors each year, the total population of the county is a mere 37,009. This number is necessary to know as it plays a part in determining new cases per 100,000 population over a seven-day period.
The first goal in achieving a low or medium Community Level is having less than 200 new COVID-19 cases over a seven-day period. For Dare County that means having 74 or fewer cases (74/37,009*100,000=199.9 cases per 100k). Counties with higher populations will be able to have a higher number of cases before exceeding 200 cases per 100,000, which is one minor example of why the tool doesn’t work well for Dare County as the county is ‘judged’ as only having 37,009 residents, but on any given week the county may have hundreds of thousands of week-long visitors.
During the entire pandemic, Dare County has reported only 27 deaths, the last occurring in Jan. 2022.
As for hospitalizations, in some cases this simply is a person going to the hospital, taking a test which proves positive and walking back out the door 15 minutes later. The person in this example would count as a new hospital admission for the entire seven-day reporting period.
Next, county hospitalizations are estimated by the CDC, even though local health departments have actual numbers. In a footnote on the CDC’s data tracker webpage, the CDC states, “data presented here use standard metrics across all United States counties. For the most accurate and up-to-date data for a specific county or state, visit the relevant state or local health department website.” This is an interesting footnote since an increasing number of agencies, businesses and schools are adopting the Community Level tool to make masking decisions and in the process are ignoring accurate local health department data.
This is when the Community Level tool gets very messy. Almost every county in America is bundled into Health Service Areas (HSA) for the purposes of determining new admissions per 100,000 population. Determining which counties are bundled together can be found here.
What does this mean? It means that a county’s Community Level destiny isn’t simply determined by its own cases and hospitalizations; a county’s destiny more often than not is hindered by hospitalizations in other counties, some of which are hundreds of miles away.
Dare County’s HSA includes three other counties, none of which share a border with Dare County. Curiously, Currituck County, N.C. shares two borders with Dare County but is located within an HSA that includes Virginia Beach, Va. Remember Dare County’s 37,009 population? Its four-county HSA has a population of 101,163. The HSA population number is critical in determining new admissions per 100,000 population.
Here are a few striking of examples of the number of hospitalizations DCHHS reported during a seven-day period compared with what the CDC reported for Dare County’s HSA.
Dare County June 16, 2022 Hospitalizations
- DCHHS reported 3
- CDC reported 12
Result: Dare County was in a high level. If Dare County used its accurate number, community level would have been medium.
Dare County July 14, 2022 Hospitalizations
- DCHHS reported 0
- CDC reported 24
Result: Dare County was in high level. If Dare County’s accurate number, zero, was used, community level would have been medium. In this example, clearly one or more of the three other counties within the HSA had a bad week. It is hard to imagine that anyone would think a county with zero hospitalizations should be in a high community level, but that’s exactly what happened to Dare County on July 14.
Dare County July 21, 2022 Hospitalizations
- DCDHHS reported 2
- CDC reported 18
Result: Dare County was in high level. If Dare County’s accurate number was used, community level would have been medium. Again, another bad week for other counties in the HSA negatively impacted Dare County.
Between June 9 and Aug. 4, Dare County had a high Community Level six out of nine weeks. If accurate hospital data reported by DCHHS was used to determine the level, Dare County would have been in medium Community Level nine out of nine weeks.
It is also noteworthy that Hyde County, N.C., located to the south and west of Dare County, was recently estimated to have had less than 10 cases during a seven-day period but during the same period was reported to have 81 hospitalizations. To repeat, the CDC reported Hyde County had less than 10 cases resulting in 81 hospitalizations. How is it possible? Hyde County, with a total population of 4,937 is in an HSA with five other counties equaling 270,709 total population. Cases are based on the county and hospitalizations are based on the HSA.
Why does any of this matter?
To most Americans that have moved on with their lives, the CDC’s Community Level tool doesn’t matter. Here are a couple of examples of the tool’s fiscal and managerial consequences.
- Most visitors to indoors facilities on federal land managed by the National Park Service and Fish and Wildlife Service, for example, no longer carry masks, so every week these Community Level tool-adopting land management agencies are spending potentially tens of thousands of taxpayer dollars on supplying masks to visitors that are unaware of a high Community Level. In the case of Dare County, N.C., masks were wrongly required for six out of nine weeks due the CDC’s reliance on HSAs and incorrect case and hospitalization data, leading to a gross waste of funds at three national park units and two wildlife refuges in the area, and forcing thousands of visitors and hundreds of federal employees to wear masks for no reason.
- Once a government agency, business or school adopts the CDC’s Community Level tool, flexibility to make masking decisions based on accurate local data and prevalence of vaccines and treatments in a local community are completely removed. Instead, the owner of a complex, inaccurate CDC database is managing all your decisions related to COVID-19.
Regarding forced mask-wearing, there may be some people who say, “It’s just a mask, just wear it for eight hours a day at work and deal with it.” However, for many people, the mask has come to symbolize where we’re at in the pandemic.
When county-level vaccination rates, decreases in deaths and decreases in the strength of variants aren’t factored into decision-making, it doesn’t inspire hope that we’ll ever get out of the pandemic.
Strict adherence to the CDC’s broken Community Level tool should be ended by all that have adopted it and all Americans should be allowed to begin a post-COVID mental health healing process. The future of our country depends on it.
Reposted from the author’s Substack
Join the conversation:
Published under a Creative Commons Attribution 4.0 International License
For reprints, please set the canonical link back to the original Brownstone Institute Article and Author.








